INTRODUCTION
Dermoid cyst can be histologically classified as dermoid cyst, epidermoid cyst, and teratoma, and it is known as proliferation of epithelial tissue of the congenital tumor, contained in the first pharyngeal arch (branchial arch) and medial epithelial seam of the second pharyngeal arch, but can occasionally be acquired [1]. Dermoid cyst is a benign congenital tumor formed by cells abnormally separated at the period of fusion of viviparous tissues. The encapsulated cyst consists of stratified epithelium lined by laminated keratin material containing adnexal structures of skin, such as sebaceous gland, sweat gland, hair follicles, and hair [1,2]. It rarely occurs in the head and neck area and 7% of the overall prevalence has been reported to occur in the peripheral orbit, oral cavity, or nasal area, or in the center of the head and neck area [2]. Epidermoid cyst is a common benign disease of the skin caused by inflammation of hair cortex follicles and proliferation of epidermal cells, and it can be congenital or acquired [3,4]. Dermoid cyst and epidermoid cyst at the auricular area are extremely rare [1]. Epidermoid cysts can also be acquired, and can be caused by various parts of the examination or after surgical operations, and in pediatric cases, determining whether an epidermoid cyst is congenital or acquired can be difficult. The authors experienced six cases of dermoid cyst and epidermoid cyst of the auricle; four cases were congenital and two cases were acquired. The cases of acquired cyst involved recurrence after surgery. In our institute, we experienced a relatively rare congenital and acquired dermoid cyst and epidermoid cyst of the auricle caused by several reasons and report different characteristics of each case with a review of the literature.
METHODS
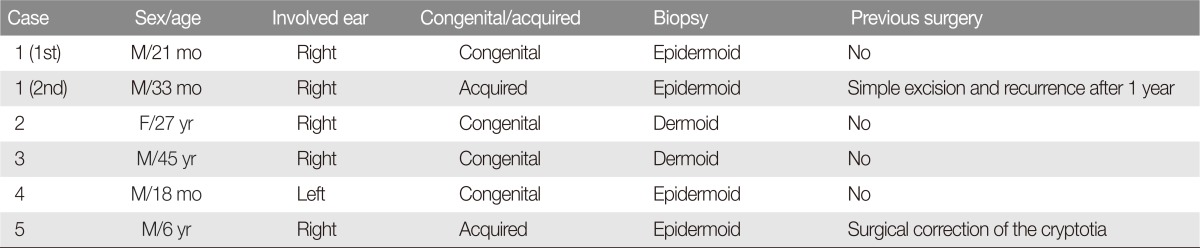
Six patients were selected among patients with an enlarged ear mass pathologically diagnosed with dermoid cyst. Four cases were congenital and two cases were acquired. One patient had a history of previous surgery for cryptotia, and the other patient had a history of excision of a dermoid cyst and was included as the congenital group in this study. Five of 6 patients underwent excision and biopsy and completed surgery without remnant tissue (Table 1).
RESULTS
Case 1
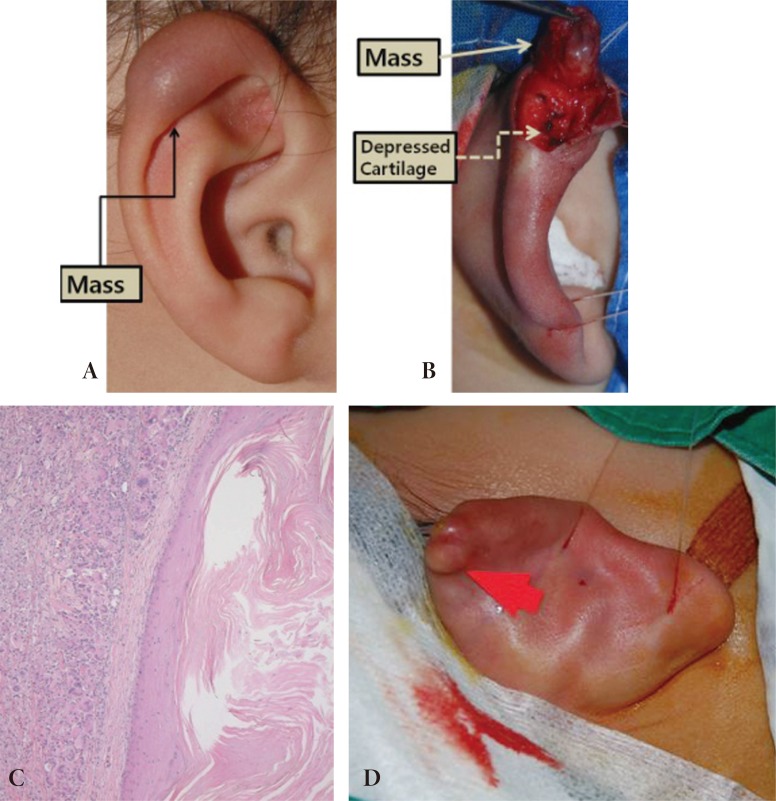
A 21-month-old boy visited the hospital with a complaint of pain and redness at the right helix with an enlarged mass. A mass on the ear had existed from birth, and the size of the mass had recently shown a slight increase. The patient had no history of trauma, family history, or other associated abnormalities. On the physical examination, an obviously raised lump measuring approximately 2├Ś2 cm in size was found at the upper part and back of the helix. The surface of skin on the mass appeared to be normal, except for a slight redness and skin findings of fistula or skin adhesions were not observed. Because this patient is a child, surgery was performed under general anesthesia with an incision parallel to the auricle and parallel to the longitudinal axis of the mass at the back of helix. Because adhesion of helix cartilage to surrounding tissues was minimal, the skin covering the mass was raised easily. Helix cartilage on the mass was removed easily, however, an unusual depression was found on the helix cartilage. The mass was encapsulated; it was a cystic mass and cheese-like sebum was observed during dissection.
Histological examination showed that the encapsulated film was composed of stratified squamous epithelium, and the inside of the cyst was composed of a keratinous cyst with laminated keratin material, however, adnexal structures of skin, such as hair and sweat glands, were not observed. Thus, it was diagnosed as an epidermoid cyst and invasion of acute and chronic inflammatory cells was observed around the mass. Skin suture was performed after excision of the mass, and no other procedure was required for treatment of depressed cartilage. Until three months after surgery, no complication such as inflammation was observed, however, at approximately one-year follow-up after surgery, two masses were observed at the top of the ipsilateral helix. The masses were removed and histologic examination showed the same result as that of the last year. Thus, the first mass was diagnosed as a congenital epidermoid cyst and the second was diagnosed as an acquired epidermoid cyst (Fig. 1).
Case 2
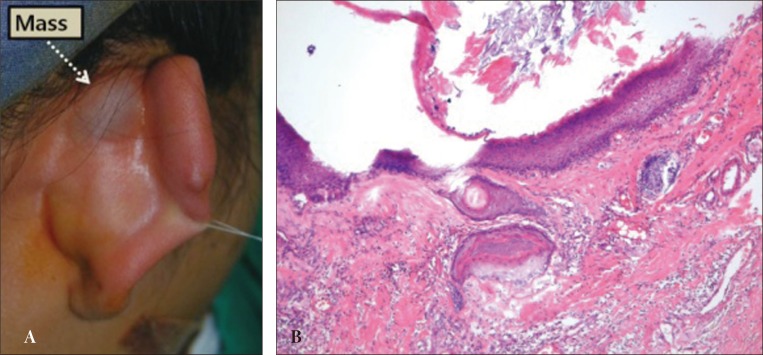
A 27-year-old woman visited the hospital complaining about the size of a mass, which measured approximately 2├Ś2 cm in size, located on the right side of the auriculocephalic sulcus since birth. The patient had no history of trauma, family history, or other associated abnormalities. The surface of skin on the mass appeared to be normal, except for a slight redness with no specific findings. Because histological examination showed that the encapsulated film composed of stratified squamous epithelium consisted of keratinous cyst with laminated keratin material and adnexal structures of skin such as hair and sweat gland were observed, it was diagnose as a dermoid cyst. Recurrence did not occur after surgery (Fig. 2).
Case 3
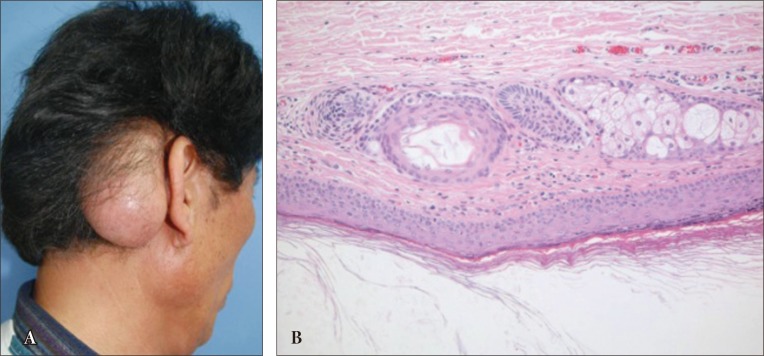
A 45-year-old man presented with a mass measuring approximately 5├Ś6 cm in size and gradually increasing in size located on the right side of the auriculocephalic sulcus and around the mastoid area. The skin and scalp on the mass were thinner due to expansion of mass size and fistula or skin adhesions were not observed. This surgery was performed under general anesthesia and encapsulated masses, including skin area, were completely resected. The mass was diagnosed as a typical dermoid cyst (Fig. 3).
DISCUSSION
Embryological dermoid cysts are assumed to occur when epithelial cells are isolated at the blockage of the pharyngeal arch of viviparous or implantation of epidermis into dermis due to penetrating injury [1]. The origin of the auricle is formed by three hillocks at each side of the head and tail of the branchial arch, which is located between the first and second pharyngeal arch at six weeks of viviparous. These hillocks will be grown to form ears at seven weeks of viviparous. Histologically, dermoid cyst is composed of stratified squamous epithelium containing sebaceous glands and hair follicles, and adnexal structures of skin, such as laminated keratin material and hair, have been observed inside the cyst. Epidermoid cyst consisting of keratinous cyst and adnexal structures of skin was not observed. The other type is teratoma, which may include organs such as ectoderm, endoderm, mesoderm and adnexal structures of skin [1]. However, all of these types are common and they contain laminated keratin material.
Ikeda et al. [2] reported two cases caused by outbreak of hillock at the auricle. These occurred since the outbreak of the auricle to form the upper part of the auricle of the fusion process of the first pharyngeal arch and to form an inclusion cyst, which causes dermoid cyst. This can be easily detected because it is located on the surface, however, it is sometimes found at the back of the helix cartilage located within the auriculocephalic sulcus. It is not found as a mass but appears as an auricle protruding toward the front but also in the form of a common mass [5]. On the other hand, the pathogenesis of epidermoid cyst has a variety of hypotheses; congenital epidermoid cyst will be caused by a shift of epithelial rests between 3 to 5 weeks of viviparous and mainly occur at the head and neck area. In the case of acquired epidermoid cyst, it is generated by blockage of hair cortex follicles, implementation of epidermis cell proliferation into the dermis due to penetrating injury [4]. The characteristic histologic array of cells at the follicular cyst wall consists of epidermal cells and granule cells in the origin of follicular infundibulum and filled with a cheese-like discharge, which is mainly fat. Therefore, it is not simply formed by trapping epidermal keratinocytes but also obstruction of the hair follicle wall just below the epidermis of skin cells, and together with sebum glands located within the papillary dermis under the skin, is known to be the main cause of epidermoid cyst; it can occur congenitally, however, an acquired epidermoid cyst causes significant confusion for both doctors and patients. In the current literature on epidermoid cysts that occurred after some kind of surgery, posttraumatic epidermoid cyst developed as a result of recent earlobe piercing of young people, and an acquired epidermoid cyst occurred after trauma through the skin from a subcutaneous scar tissue component of the trauma caused by accidental implantation. Epidermoid cyst after foreign body implantation or injection therapy or after cosmetic surgery has been reported [3,6]. Cystic lesions occurring in the ear as a differential diagnosis are histologically dermoid cyst, epidermoid cyst, cystic teratoma, lipoma, hemangioma, branchial cyst, trichilemmal cyst, and keloids, and so on [1,3,7]. Most dermoid cysts at the auricle undergo surgery due to cosmetic reasons and surgery can also be performed for compression or irritation on the surrounding tissues and induction of inflammation. Incomplete removal may result in recurrence or infection, thus, complete surgical excision is necessary [1,3,6].
The author experienced six cases in five patients with dermoid cyst and epidermoid cyst in the area of the ear. Congenital dermoid cyst occurred in four cases, and there were two cases of acquired dermoid cyst. Histologically, we had two cases with dermoid cyst and four cases with epidermoid cyst. Among four cases of congenital epidermoid cyst, three cases had a feature located on top of the helix. On the other hand, in the two cases of dermoid cyst, a mass was found at the auriculocephalic sulcus or back of the helix. The first three patients with epidermoid cysts were children with no history of trauma or surgery, thus, it is believed to be congenital.
In case 1, epidermoid cyst possibly occurred over a period of 4 to 5 weeks in the first and second pharyngeal arch of six globules that fused together and ectodermal component was depressed between two and three prominentia The cyst was diagnosed histologically as an epidermoid cyst instead of a dermoid cyst, which can cause retardation in growth and development resulting in less developed adnexal structures of skin at the cysts. In addition, depressed cartilage can be observed at the bottom of the mass; this could be of the adjacent portion of bone of dermoid cyst accompanied by depressed bone. Even considering differences between the cases, this strongly suggests that epidermoid cyst occurred congenitally. Two cases occurred as acquired, the first case occurred one year after surgery for a congenital dermoid cyst, and the other case was an acquired epidermoid cyst after corrective cryptotia surgery. The first case was inflammation after surgery, possibly caused by residual tissues or cyst during the surgery and the possibility of remaining skin tissues or cystic tissues at perichondrium located at the bottom of the mass, and the possibility of surgical incision and engraftment of skin cells during the surgery was also considered. Therefore, surgery of these dermoid cysts requires close attention with control of inflammation. Finally, two cases of dermoid cyst were located at the auriculocephalic sulcus or back of the helix connecting to the hair part. It was considered to be looking at the occurrence of the auricle, which is formed within seven weeks of viviparous, when the auricle occurs for formation of the upper part of the helix of the fusion process of the first pharyngeal arch and in the surrounding tissues that formed an inclusion cyst that causes dermoid cyst.
Kim et al. [3] experienced an acquired dermoid cyst, and did not report a difference between congenital dermoid cyst and acquired dermoid cyst. Unlike a congenital dermoid cyst surrounded by normal tissues, an acquired dermoid cyst was isolated, and surrounded by fibrous scar tissue. In addition, in this study, location of the mass has a significant value as it is associated with the occurrence of the auricle with the diagnosis of dermoid cyst at the ear. Particularly, in the case of an epidermoid cyst, history is important because it is difficult to prove histologically whether the cyst is congenital or acquired in the differential diagnosis. The authors emphasize that trauma or surgical procedure can cause acquired epidermoid cyst or acquired dermoid cyst, thus, a careful approach is required for access and report with literature review.