Odontomas are a common type of odontogenic tumor. Histologically, an odontoma is considered to be a hamartoma rather than a neoplasm. The majority of odontomas are asymptomatic, although swelling, pain, bony expansion, and displacement of teeth have been infrequently observed [1]. Most patients with odontomas are managed by dentists for simultaneous management of associated dental problems, but some tumors are incidentally discovered by plastic surgeons while examination of the jawbones for trauma. We present the management of such a case of incidentally discovered odontoma.
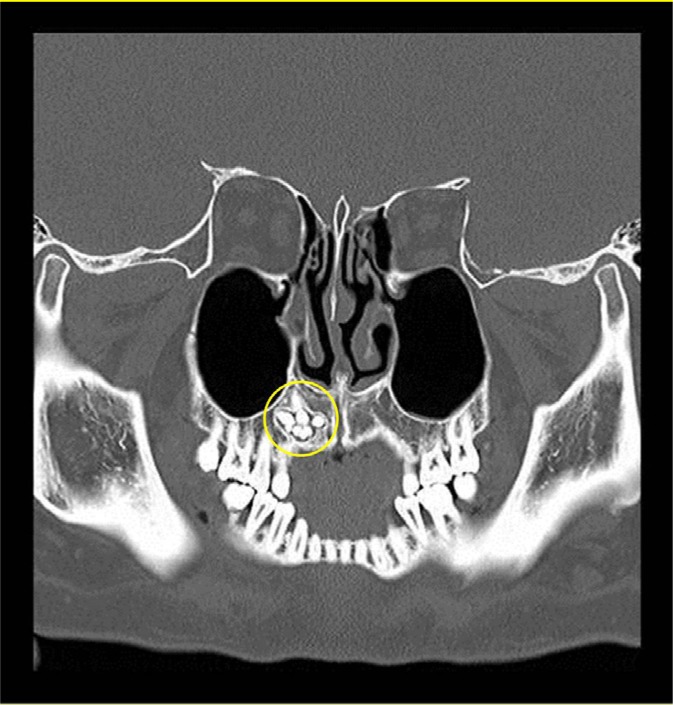
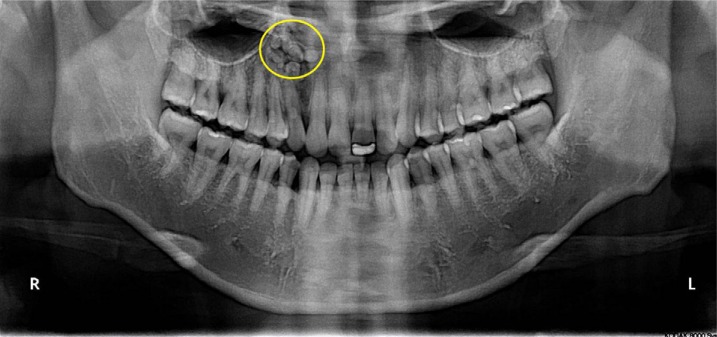
A 38-year-old male presented with right facial contusion after an altercation. Computed tomography (CT) did not identify any facial bone fractures but revealed multiple tooth-shaped structures within the alveolar process of the right maxilla (Fig. 1). Panoramic X-ray showed these structures to be of varying shapes and sizes near the root of the right upper canine tooth (Fig. 2). Each structure was surrounded by well-circumscribed radiolucent zone. Having been alerted to the incidental discovery, the patient stated that the right upper gum had been bulging for the past year but did not seek medical attention as it did not cause him any discomfort. On examination, the right upper alveolar ridge was nontender, and the overlying mucosal lining was of normal color and consistency.
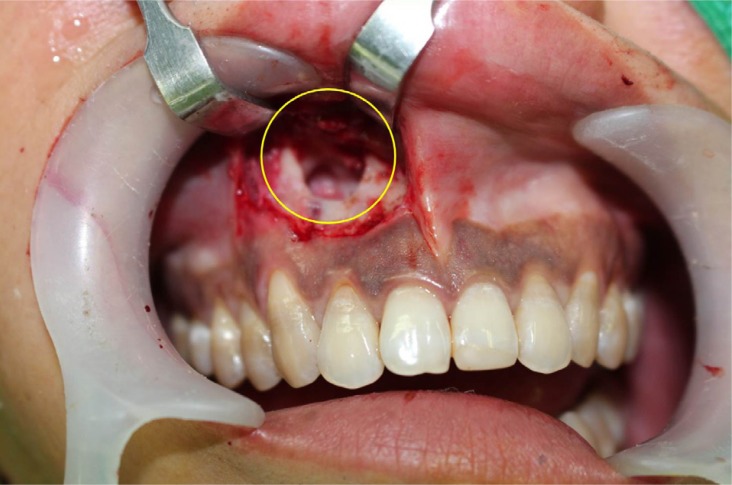
Under local anesthesia (2% xylocaine with 1:100,000 epinephrine), a gingivobuccal mucoperiosteal flap was elevated from central portion, and a bone flap was temporarily removed for access to underlying odontoma. Once the space was accessed, multiple denticles were enucleated along with the fibrous capsule (Fig. 3). After sufficient curettage of mucosal lining and dysplastic tissue, the remaining space were filled with 1 mL of demineralized bone matrix (DePuy Synthes Inc., Los Angeles, CA, USA). The bone flap was returned to the original position, and the mucosa was closed with 5-0 Vicryl suture.
A total of 11 denticles were enucleated. There was no concrescence or fusion. The denticles varied in size from 3 to 10 mm (Fig. 4). Histologic examination showed miniature teeth containing dentin with dentinal tubules, pulp, cementum, and periodontal ligament-like tissue, which were all findings suggestive of compound odontoma (Fig. 5). At 10-month follow-up, the mucosal surface had healed with no signs or symptoms of bony resorption or recurrence on radiographic study.
Odontoma is a benign tumor that arises from normal dental tissue. While the tumor represents about 22% of all odontogenic tumors, the population incidence is less than 0.1% [2,3]. According to the 2005 classification by the World Health Organization, odontomas are distinguished between compound and complex types, depending on the morphology. Compound odontomas are formed by small tooth-like structures which resemble pulp tissue in the central portion and surrounded by a dentin shell and enamel. Complex odontomas are conglomerates without orientation of dentin, enamel, cementum, and pulp tissues. Compound odontomas are more commonly found in anterior maxilla, whereas complex odontomas tend to occur in posterior maxilla or mandible [4].
Odontomas are generally small, and patients are asymptomatic. Occasionally, an odontoma can present as a large mass with bone expansion, impaction, and delayed eruption of either primary or permanent teeth [5]. In such cases, surgical removal might be a challenge. After enucleation of denticles and associated soft tissue, proper reconstructive options should be selected for a satisfactory outcome. Small, localized odontomas are relatively easy to manage, but large odontomas may require a complex reconstructive approach which includes osteoplasty, soft tissue reconstruction, and dental prosthesis.