INTRODUCTION
Solitary fibrous tumor is a tumor of mesenchymal origin that was first described by Klemperer and Rabin [1] and is known to occur mainly in the pleura. It has also been reported to develop in various other locations, however, such as the abdominal cavity, upper respiratory tract, and soft tissue, but its occurrence in the oral cavity is extremely rare, and there have been few reported cases of such in South Korea. Solitary fibrous tumor can be treated by surgical excision, and immunofluorescence staining is employed for differential diagnosis with factors like CD34 and CD99. In the authors' Department, there has been one case of diagnosis with solitary fibrous tumor after total resection and histopathologic examination for a buccal cheek mass. Such rare case is reported herein.
CASE REPROT
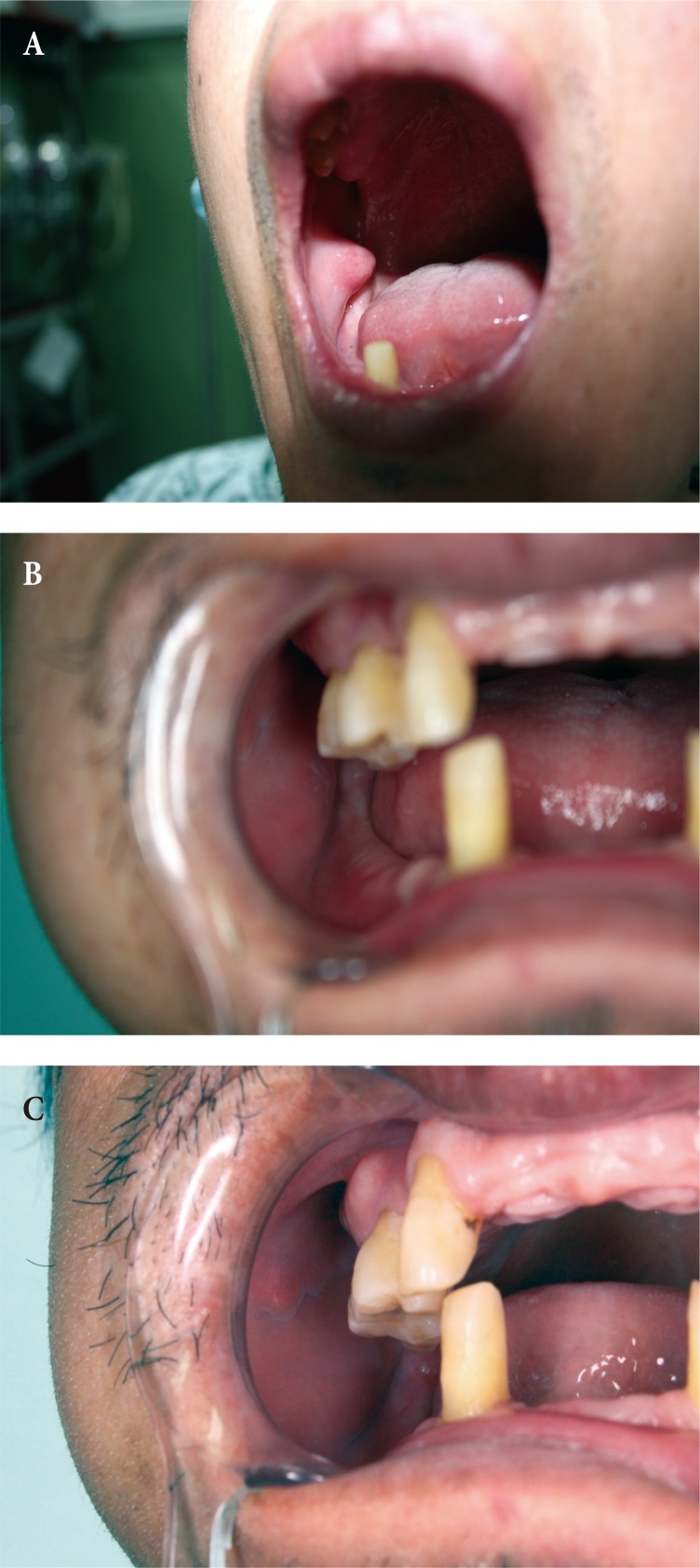
The patient was a 50-year-old man with a touchable mass in the buccal mucosa of the right cheek who visited the Plastic Surgery Outpatient Department of Dong-A University Hospital as the size of the mass had become larger. The patient did not have any unusual condition, except for histories of open reduction and internal fixation for LeFort I & II fracture due to falling. The patient thought that the mass developed after he incurred such injury. There was no specific finding at the visual inspection, and a soft-tissue lump that felt slightly hard was touched upon palpation. In the mouth, an approximately 2 cm mass covered by normal mucosal tissues was uplifted (Fig. 1A). Under local anesthesia, excisional biopsy was performed, and after the complete removal of the lesion, the surgical site was sutured. The tissue that had been removed had clear boundaries and was covered with a fibrous capsule. The mass was well demarcated, oval, and 1.5 cm in size, showing a diffuse fibrotic appearance. The tissue that had been obtained through the surgery was fixed in 10% formalin, and hematoxylin & eosin (H&E) staining and immunofluorescence staining were done. In the H&E staining, the mass was found to have been composed of abundant collagenous stroma admixed with bland-looking tumor cells (Fig. 2). In the immunofluorescence staining, positive responses to CD34 and CD99 (Fig. 3) and negative responses to Bcl-2, S-100, and smooth muscle actin (SMA) were shown. There was no finding of inflammation or recurrence 3 months and 5 years after the surgery (Fig. 1B, C).
DISCUSSION
Solitary fibrous tumor is a tumor of mesenchymal origin and is known to occur mainly in the pleura but also occurs in the peritoneum, pericardium, and mediastinum. It was recently reported to have occurred in the epithelial organs, such as the thyroid, paranasal sinus, orbital soft tissue, lacrimal gland, and skin [2,3,4]. In the 153 cases of solitary fibrous tumor that developed in the head and neck that were examined by Cox et al. [5], 26.1% developed in the buccal mucosa, 9.2% in the nasal cavity, 7.8% in the pharynx, 7.2% in the tongue, and 6.5% in the orbit. Solitary fibrous tumors in the head and neck are relatively rare compared to other sites. As there are not many cases, there are no definite diagnosis criteria, but they can be diagnosed via computed tomography (CT), magnetic resonance imaging, and positron emission tomography-CT. Neurofibroma, schwannoma, leiomyoma, and hemangiopericytoma are the lesions that need to be differentiated. For differential diagnosis, H&E staining and immunofluorescence staining are used.
Through H&E staining, the cell array pattern in the solitary fibrous tumor can be observed. The cell array pattern is characterized by various findings, including the arrangement of fusiform cells with a histologically relatively regular shape and size but without a particular form, a swirling growth style, the appearance of enlarged vessels observed in the mesothelioma of the blood vessels, fibrosarcoma-shaped growth, and a substrate with a low cell density and with enriched acidophil fibers [6]. In immunofluorescence staining, a positive response to CD34 is shown, and mast cells are shown to be abundant in the solitary fibrous tumor because such tumor originates from a CD34-positive pluripotential cell. CD99 is also known to be helpful at the time of diagnosis because the solitary fibrous tumor shows positive responses in varying degrees. The CD34 antigen is a single-chain glycoprotein inside and outside the membrane of 115 kDa that is selectively expressed in human hematopoietic progenitor cells and endothelial cells. It is also found in the mesenchymal and interstitial cells and in various types of mesenchymal tumors [7].
In the case reported herein, positive responses to CD34 and CD99 and negative responses to Bcl-2, S-100, and SMA were shown. Neurofibroma and schwannoma may be positive to CD34 and Bcl-2 but is negative to S-100; thus, they can be easily differentiated. Leiomyoma is positive to SMA but is negative to CD34 and Bcl-2; thus, it can be easily differentiated. It should be noted that CD34 is expressed not only in solitary fibrous tumor but in many other types of tumor cells, such as the dermatofibrosarcoma protuberans, spindle cell lipoma, and hemangiopericytoma. As a result, it is difficult to use CD34 as a specific marker of solitary fibrous tumor. Moreover, Vimentin, Bcl-2, CD99, and Factor XIIIa are also expressed in other tumor cells. Therefore, there is no solitary-fibrous-tumor-specific marker to date, and it is necessary to make a diagnosis by comprehensively considering the histologic findings and expressions of various markers [8].
As the solitary fibrous tumor usually grows slowly and without pain, the patient is often not aware of its presence until it has grown to a certain size. In the case of a solitary fibrous tumor that developed in the mouth, in most cases, the patients visit the hospital with a major complaint of dysarthria or masticatory disorder [9].
Solitary fibrous tumor is treated by surgical total resection. Most tumors are benign, and the prognosis is known to be good. Most solitary fibrous tumors show a single type of tumor cell proliferation findings, but malignant findings may also be shown in a few cases. If cell polymorphism, high cell fidelity, a number of division patterns (4 or more in high-magnification findings), and necrosis of the tumor cells are shown, the possibility of malignant degeneration should be considered, and association with a high recurrence rate and distant metastasis is indicated [10]. In addition, more malignant cases of solitary fibrous tumor in the extremities have been reported in another study [11]. If malignancy is suspected based on the biopsy finding, a more aggressive treatment should be considered, such as wide excision. The case reported herein was judged as a benign tumor, and recurrence was not observed 5 years later, but as it may recur, long-term follow-up is necessary [9].
Reported herein is a resolved case of a 50-year-old male patient with a facial fracture history who visited the hospital with a major complaint of a subcutaneous mass that had developed in the buccal mucosa on his right cheek. After the performance of total resection under the suspicion of the presence of a mucosal polyp or fibroid that had developed due to the patient's previous injury, solitary fibrous tumor was diagnosed as a result of the biopsy that was conducted. As the development of solitary fibrous tumor in the buccal mucosa is extremely rare in the South Korean medical literature, the case was reported along with a literature review.