INTRODUCTION
Ultrasonography is a useful noninvasive method to detect the exact location of subcutaneous tumors before surgery. However, findings are not always in accordance with the actual echogenicity of the soft tissue mass. Importantly, there is a possibility of misdiagnosis atypical cases when using ultrasonography.
Intraosseous hemangioma is a rare, slow-growing, benign tumor of blood vessels accounting for 0.7% of all neoplasms of bone [1]. Meanwhile, calvarial hemangiomas, which account for 0.2% of all bone neoplasms, are more than three times more common in women than men. Although calvarial hemangiomas can be seen at any age, patients are usually treated between 20 and 40 years of age [2]. Intraosseous hemangiomas are most commonly found in the vertebral column and rarely seen in the calvarium. Among the calvarial bones, the parietal bone is the most commonly involved; frontal, occipital and temporal bones are less frequently involved [3]. The intraosseous calvarial hemangiomas may be monofocal or multifocal, but the majority of reported cases are monofocal. In very rare cases, multifocal hemangiomas may occur [4].
CASE REPORT
History and presentation
A 60-year-old male patient presented with a complaint of a painless palpable mass in the left forehead region that had been slowly enlarging for past 2 years. There was no history of forehead trauma. Medical and surgical histories were insignificant.
Physical examination
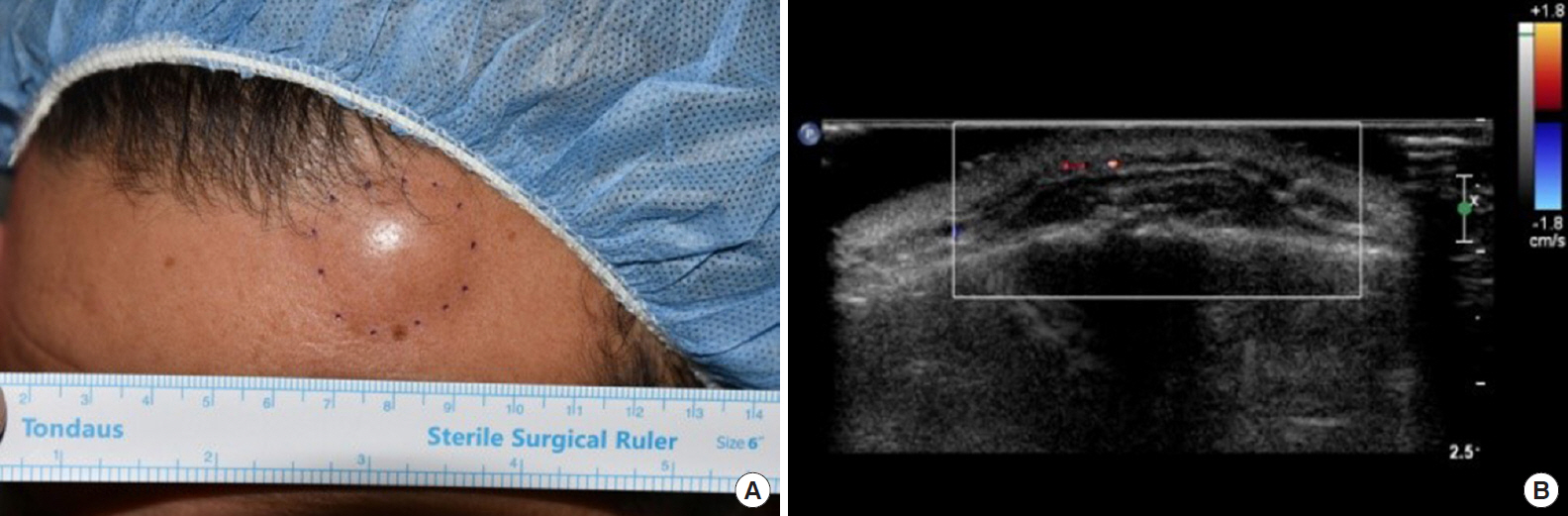
On physical examination, swelling (diameter, 2.5 cm; height, 7 mm) was observed without change of the overlying skin in the left forehead area (Fig. 1A). The swelling was not so firm, non-fluctuant, non-tender and slightly movable without any bruit. There was no change in size with compression. The head shape was symmetric. There were no other abnormal findings upon general and neurologic examinations.
Radiologic imaging
Ultrasonography revealed a well-defined margin adjacent to the left frontal bone in the subgaleal layer, with a hypoechoic lesion (2.2 cm├Ś0.3 cm). Hyperechoic inside septation and focal cortical discontinuity were also observed, while the underlying bone cortex appeared relatively intact. No significant flow is observed on Doppler sonography, suggesting no evidence of internal vascularity (Fig. 1B). Thus, the mass was interpreted as a subgaleal lipoma by a radiologist.
Excisional biopsy
Complete excision was conducted under local anesthesia. The left frontal lesion was well delineated at subgaleal layer and the mass was reddish brown in color and appeared to originate from bony cortex. This lesion was attached to the outer cortex of the frontal bone and revealed hemorrhagic features with a cluster of small vessels. After excision of the mass, the cortical bone was relatively intact, but there was erosion of the outer table of the skull (Fig. 2A). To prevent possible bone bleeding, careful hemostasis with electrocauterization was performed. The mass of left frontal lesion was soft, well delineated, reddish brown, and shows hemorrhagic features with multiple vascular channels (Fig. 2B).
Additional radiologic imaging
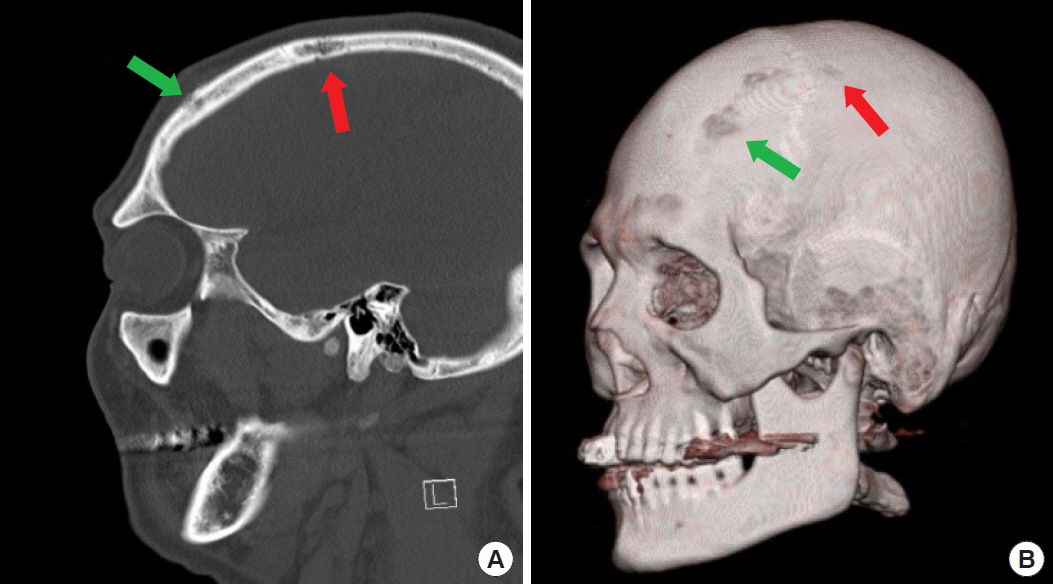
Postoperative computed tomography (CT) scans were performed due to concern about the underlying bone lesions and revealed a mild expansile nature of the mass that expanded in the diploic space in the left frontal bone. In the underlying calvarium of the parietal bone, there was multifocal partial thickness erosion presenting as a honeycomb-shaped geographic osteolytic lesion without neuroparenchymal involvement or discontinuity of the cortical surface on the outer table of the skull. A postoperative CT scan showed the presence of a multifocal intraosseous hemangioma of the parietal bone that did not connected the surgical site (Fig. 3A). Three-dimensional volume rendering technique reconstruction imaging further supported this finding (Fig. 3B). We identified a characteristic ŌĆ£scalloping signŌĆØ (depression in the outer or inner table of the skull) of the underlying frontal bone, which was the operation site, and identified a multifocal lesion in the parietal bone (not at the site of operation).
Histologic findings
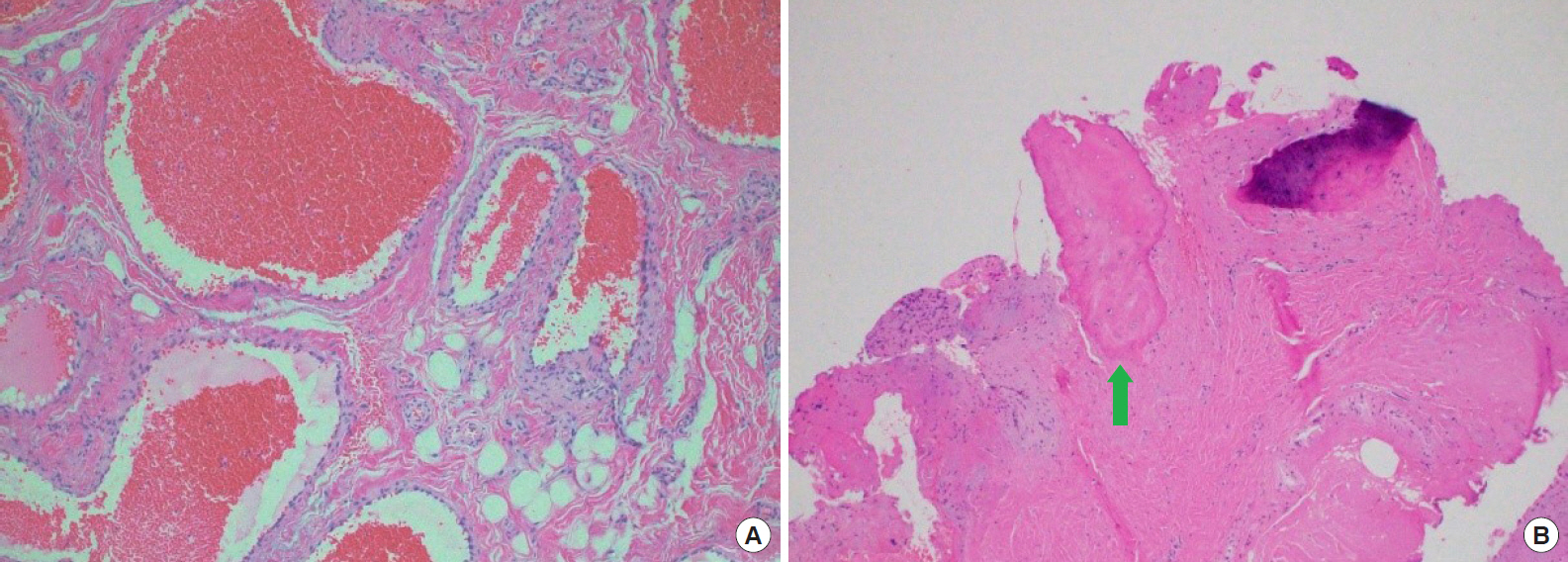
Histopathologic examination revealed a mixture of fat, loose fibrocollagenous tissue with extended, thin-walled large dilated veins filled with erythrocytes and sinuses lining a single layer of endothelial cells (Fig. 4A). The pathological features were consistent with a diagnosis of previously known cavernous hemangioma (slow-flow vascular malformation). Multiple small bony trabeculae were also revealed (Fig. 4B).
We presented the CT findings to the patient and recommended total excision and cranioplasty, however, he refused additional surgery. Instead, we recommended periodic imaging studies and removal of the mass if the size of mass increased or the inner table of calvarium becomes more osteolytic. The postoperative course was uneventful and the contour of the left forehead was well restored.
DISCUSSION
Primary intraosseous hemangioma is a benign lesion that is typically asymptomatic; occasionally, however, these lesions may appear as a slow-growing hard palpable mass with discomfort, pulsatile sensation or are accidentally detected during image evaluation [5]. The pathogenesis of primary intraosseous hemangioma remains unknown. The causes are considered congenital or traumatic, but this has not yet been proved. Etiology of hemangiomas is not yet known, but trauma history seems to be related in some previously reported cases [3]. Because these tumors tend to expand externally rather than internally, neurologic deficits are uncommon. However, Kanu et al. [6] reported that calvarial hemangioma rarely causes seizure in relation to neurological deficit.
Intraosseous calvarial hemangioma is characteristically recognized in diploic space. They are expansile in nature, widening the diploic space and causing thinning both inner and outer tables of the skull [7]. CT is the most accurate tool for determining the intraosseous range and the involvement of soft tissue (intracranial vs. extracranial location and extent). Characteristic scallops (depression in the outer or inner table of the skull) have been described to distinguish the extracranial and intracranial origins of these lesions. The extracranial lesions produce depression in the outer table of the skull and intracranial lesions produces depression in the inner table of the skull. The CT findings of intraosseous hemangioma may appear as an osteolytic defect with ŌĆ£soap bubble,ŌĆØ ŌĆ£honeycombŌĆØ or ŌĆ£sunburstŌĆØ appearances. ŌĆ£HoneycombŌĆØ appearances correspond with a scattering of radiodense spots in the radiolucent hollow [6-8]. This radiologic finding is due to osteolytic activity of the mass and secondary reactive osteoblastic remodeling with trabecular bone. Therefore, the differential diagnoses for intraosseous hemangioma include fibrous dysplasia, osteoma, Langerhans cell histiocytosis, and multiple myeloma [3].
Microscopically, multiple engorged vascular elements interspersed among abundant trabecular bones were observed in our patient. The vessels are thin walled and lined with a single endothelial layer [2]. An agglomerate of thin-walled and dilated blood vessels infiltrates the bone, while plump endothelial cells are lined inside the small-caliber thin-walled vessels [1,9].
The treatment of choice for an intraosseous hemangioma is en-bloc resection to the appropriate normal bone margin; the bone defect can be reconstructed in various ways. The others include curettage, radiotherapy, and embolization. The patient in our case did not want to undergo additional treatment, but if the size of the lesion increases on a periodic follow-up, or if the thickness of the inner or outer table of calvarium decreases, total excision of the tumor is recommended.
According to the International Society for the Study of Vascular Anomalies classification system, venous malformation (VM) has been mistakenly called cavernous hemangioma and cavernous angiomas; these terms have led to confusion with the more common proliferating or true hemangioma of infancy for many years. VM is a slow-flow vascular malformation seen at birth, however, it may typically become evident and more prominent as the patient grows up. The most pronounced enlargement is usually seen at the period from infancy to puberty, but less changes may be seen into adulthood [10].
Ultrasonography is the first-line approach to assess soft tissue masses. It can help confirm the presence of a tumor and anatomical location, extent and its relationship to the investing fascia, neurovascular bundle and other tissue without the use of ionizing radiation. Ultrasonography accuracy in diagnosing slow-flow vascular malformations is high when presenting with typical appearance. The sensitivity and specificity of ultrasonography for confirming and diagnosing VM are 73% and 98%, respectively. However, as in our case, VM is often misdiagnosed as a lipoma when the vascular malformations are of very slow flow and it is composed of mainly echogenic stroma interspersed with small capillaries that are too small to be resolved by ultrasonography [11]. As ultrasonography findings in our case, hypoechoic contents with hyperechoic linear septa can be diagnosed as fibrolipoma, and about 15% of all lipomas are hypoechoic compare to adjacent fat [12].
We present a rare case of multifocal intraosseous calvarial hemangioma arising in the subgaleal plane causing scalloping of the underlying calvarium in an elderly male patient. Biopsy for intraosseous lesions, of course, is the most accurate, but there was a limitation because the patient did not want to receive any further procedure. In histologic findings of hemangioma including bony trabeculae, we would not be sure whether some of the intraosseous hemangioma is involved in the tissue or whether the subgaleal hemangioma contains part of the cortical bone. However, there were somethings to consider in our case: intraoperative finding also showed that there were multiple vascular channels with bone bleeding, which led us to believe that the subgaleal lesion was connected inward. And the outer table of the underlying cortical bone with a hemangioma on CT was very thin. Considering these points, the authors made a diagnosis this would be intraosseous hemangioma. This case highlights the importance of additional CT examination in patients presenting with signs of underlying calvarium scalloping and erosion. Clinicians should also be aware of the possibility of multifocal intraosseous calvarial hemangiomas in lesions that may extend to the periphery and the possibility of intracranial extension, especially in the frontal and parietal bones. Furthermore, proper selection of congenital vascular malformation terminology is still quite confusing and misconception are present in the literature.