INTRODUCTION
Rhinophyma is a rare and painless benign tumor of the skin of the nose characterized by hyperplasia of the sebaceous glands, connective tissue, and blood vessels [1]. Rhinophyma is generally confined to the lower nose and does not involve the bone or cartilage framework. However, giant rhinophymas distort the nasal aesthetics, and severe cases may cause airway obstruction, thereby compromising the patientâs quality of life and emotional state [2]. There is no gold standard treatment for Rhinophyma; however, surgical treatments, such as scalpel excision, dermabrasion, cryosurgery, argon laser, carbon dioxide laser, and electrocautery, have been used to treat rhinophyma, and different treatments are applied depending on the patientâs condition [3]. A dermabrader has the advantages of low cost and precise contouring around the nose. However, not many hospitals are equipped with this device nowadays, as other techniques have been developed for treating scarring, wrinkles, and pockmarks. However, drills and burs, which function under similar principles, are widely used in plastic surgery, and are commonly available in hospitals. In this paper, we present a rare case of rhinophyma in an Asian patient who was treated at no additional cost using a bur widely used in plastic surgery.
IDEA
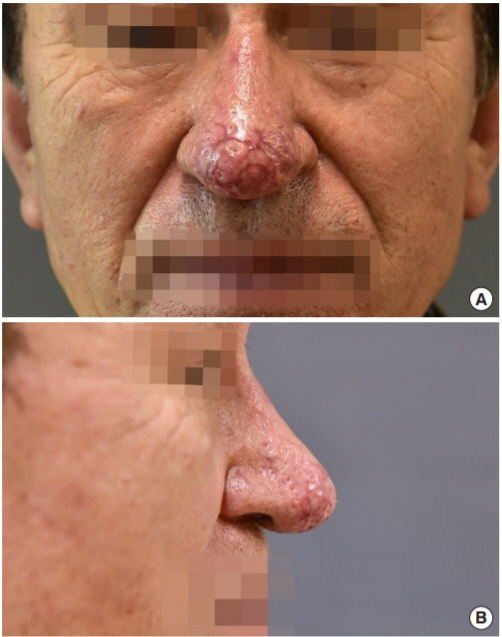
The patient was a 72-year-old man with a 10-year history of telangiectasia and erythema of the nose and a 2-year history of induration, prominence, and thickening of the nasal tissues. Although there was no pain, the patient presented to our outpatient clinic because the compressed nares caused difficulty in breathing, and it was aesthetically unpleasant. The lesion affected the nasal bridge and had spread to the bilateral alar lobules (Fig. 1). Results of a biopsy performed at the outpatient clinic suggested rhinophyma; based on this, the patient was scheduled for surgical intervention.
The surgery was performed under general anesthesia. The resection areas were designed with consideration of the nasal aesthetic unit. A mixture of 150 U hyaluronidase in 30 mL of 1:100,000 lidocaine/epinephrine was infiltrated. Then, the tumor was debulked with a #15 scalpel, followed by nasal tip contouring using a round diamond bur (Fig. 2). Contouring was performed at a bur rotation speed of 30,000 revolutions per minute (rpm). We preserved the pilosebaceous appendage for spontaneous re-epithelialization and took precautions to avoid injury to the nasal cartilage. After achieving hemostasis using Bosmin gauze, a Vaseline wet dressing was applied. Postoperatively, the dressing was changed once every 2 days. The wound was re-epithelialized 2 weeks after surgery. During 8 weeks of observation after surgery, there were no side effects, such as inflammation, and the patient was very satisfied not only with the ease of the procedure but also with the aesthetic result (Fig. 3). The nasal height, measured from the vertical alar plane to the nasal tip, was reduced by 20% after surgery.
DISCUSSION
Rhinophyma is a benign tumor of unknown cause that grows very slowly, and its worldwide incidence and prevalence remain unknown. There are only about 20 cases reported among Asians [4]. Although the exact cause of rhinophyma remains elusive, excessive alcohol intake, vitamin deficiency, repeated infections, and sunlight exposure have been suspected as risk factors [4,5]. Rhinophyma is the most severe form of rosacea, developing in the course of prerosacea, vascular rosacea, and inflammatory rosacea, and it is clinically characterized by telangiectasia, thick skin, palpable nodules, enlarged pores, and foulsmelling sebum secretion in the lower nose [6]. This slow progressive process begins in the teenage years or the twenties with rhinophyma generally diagnosed in the sixth decade of life [4,6].
Although unusual, a malignant skin tumor may develop in the thickened tissue of rhinophyma; hence, a pathologic exam is essential. Basal cell carcinoma, squamous cell carcinoma, sebaceous carcinoma, and angiosarcoma have been reported, with basal cell carcinoma being the most common [7]. In this case, the biopsy results confirmed the absence of malignant tumors.
There have been reports that nonsurgical treatments, such as topical metronidazole, retinoids, low dose isotretinoin, and oral antibiotics, were effective in treating rhinophyma. However, these treatments cannot regress rhinophyma once it progresses. Giant rhinophymas are generally treated surgically with scalpel excision, dermabrasion, cryosurgery, argon or CO2 laser surgery, or electrocautery excision [3]. A variety of other surgical interventions, such as the ultrasonic scalpel, disposable razor, PlasmaBlade, Versajet, or a combination of existing techniques, have also been attempted. However, there is no gold standard technique, and several factors, including size and location of the lesion, hemostasis, scar formation, procedure duration, and cost associated with each instrument must be taken into consideration [3,8-11].
The advantages of scalpel excision and dermabrasion include low cost and precise contouring around the nasal aesthetic unit. In this case, we first performed mass debulking with a scalpel. In contrast to existing techniques, we used a bone drill and diamond bur, which are used in bone surgeries, for contouring. A dermabrader was used by attaching a handle and diamond fraise or wire brush to a power source. A diamond fraise (Fig. 4) has recently gained popularity owing to its ability to produce even depth easily [12]. A dermabrader can operate at 10,000â85,000 rpm and is more effective at a higher speed [12,13]. While dermabraders have been used to treat scars, wrinkles, and pockmarks in the past, with the drastic decrease in smallpox cases and advances in laser therapy, not many hospitals today are equipped with this device. In contrast, drills, and burs, which operate under a similar principle, are widely used in plastic surgery and are commonly available in hospitals. Generally, when cutting bone, a carbide bur is preferred and a diamond bur is mainly used to smooth the rough surface of the bone (Fig. 4). We can perform surgery at no additional cost by using an ordinary bur which we already possess.
Difficult hemostasis and severe scar contracture may develop if the entire dermal layer is injured by inappropriate depth control [3,5,6]. It is important to preserve not only the cartilage framework but also the pilosebaceous appendages to allow reepithelialization. We therefore set the speed of our drill to its maximum of 30,000 rpm for precise depth control, and used a small round diamond bur for the delicate contouring of the nasal aesthetic unit.
However, in this case, we were able to control bleeding by injecting a vasoconstrictor prior to excision and using hyaluronidase, which promotes the spreading of the locally injected solution. This not only led to more effective hemostasis but also lowered distortion after injection [14]. There have been reports of using the latest instruments to treat rhinophyma. However, along with relevant literature review, we present a case of giant rhinophyma treated effectively at no additional cost using only bone surgery equipment.