INTRODUCTION
Pixie ear is a noticeable deformity [1] that appears as an attached, tapered, and low-set earlobe [2]. It can be congenital or acquired, and acquired causes include trauma, rhytidectomy, or total reconstruction of the ear [1,3,4]. Traditional methods have been reported, but they usually excise the lobule and reattach it in a superior position [5,6]. The scar along the border of the earlobe, however, disturbs the earŌĆÖs natural appearance and can become hypertrophied [6]. In addition, the surgery is combined with fat or dermofat graft in the earlobe [7] and performed with complicated plication suture around the earlobe [2].
The present report suggests a simple skin redraping method for correction of pixie ear without a visible scar. This concept is modified and based on medial epicanthoplasty using the skin redraping method [8]. Like skin redraping epicanthoplasty removes the hood of the epicanthal fold and expands the medial canthus, skin redraping correction of pixie ear removes the hood of the pixie earlobe and forms an intertragal notch between the earlobe and the jaw line. Furthermore, the scar sits in the retroauricular area and is inconspicuous when viewed from the front.
IDEA
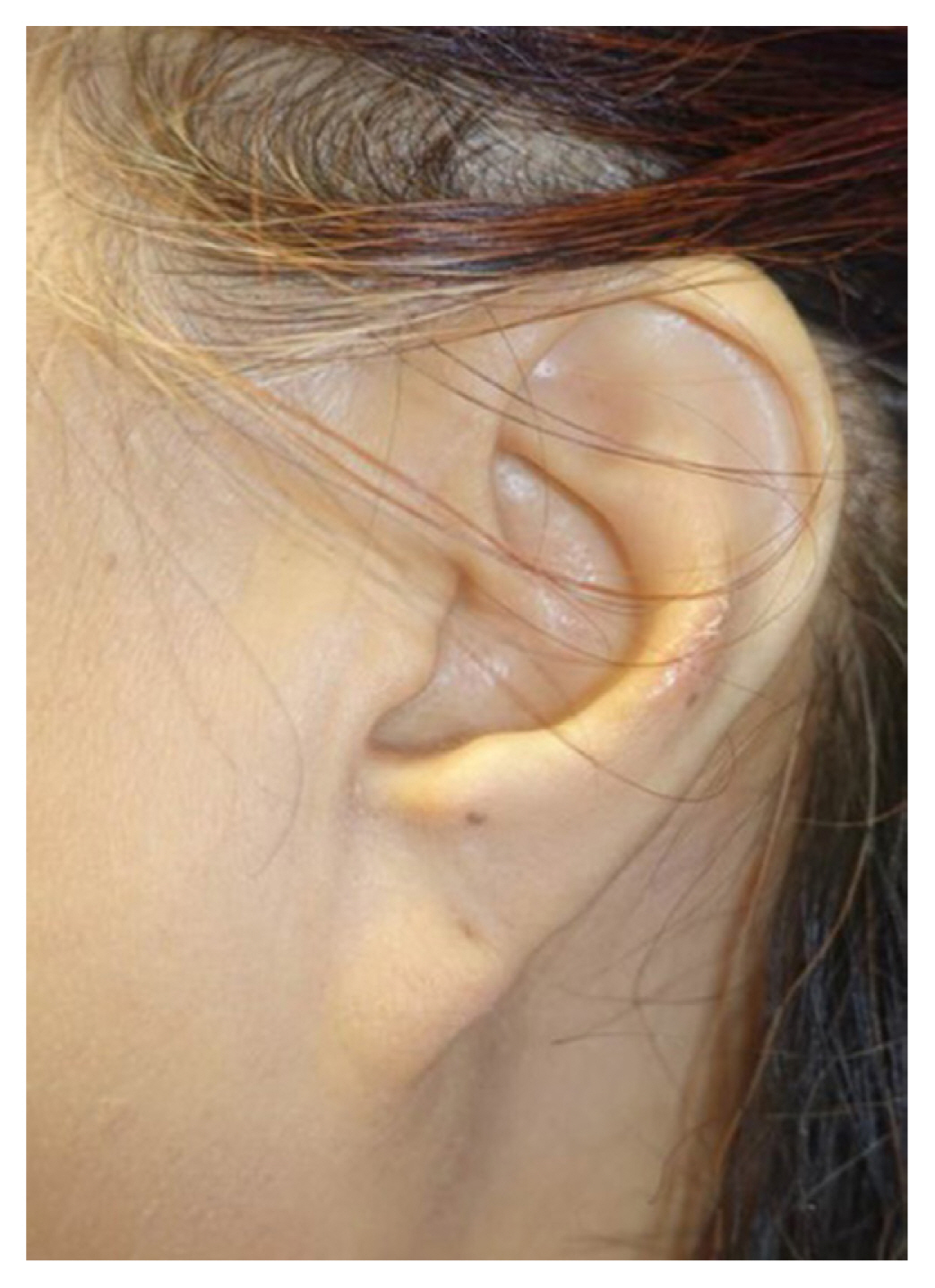
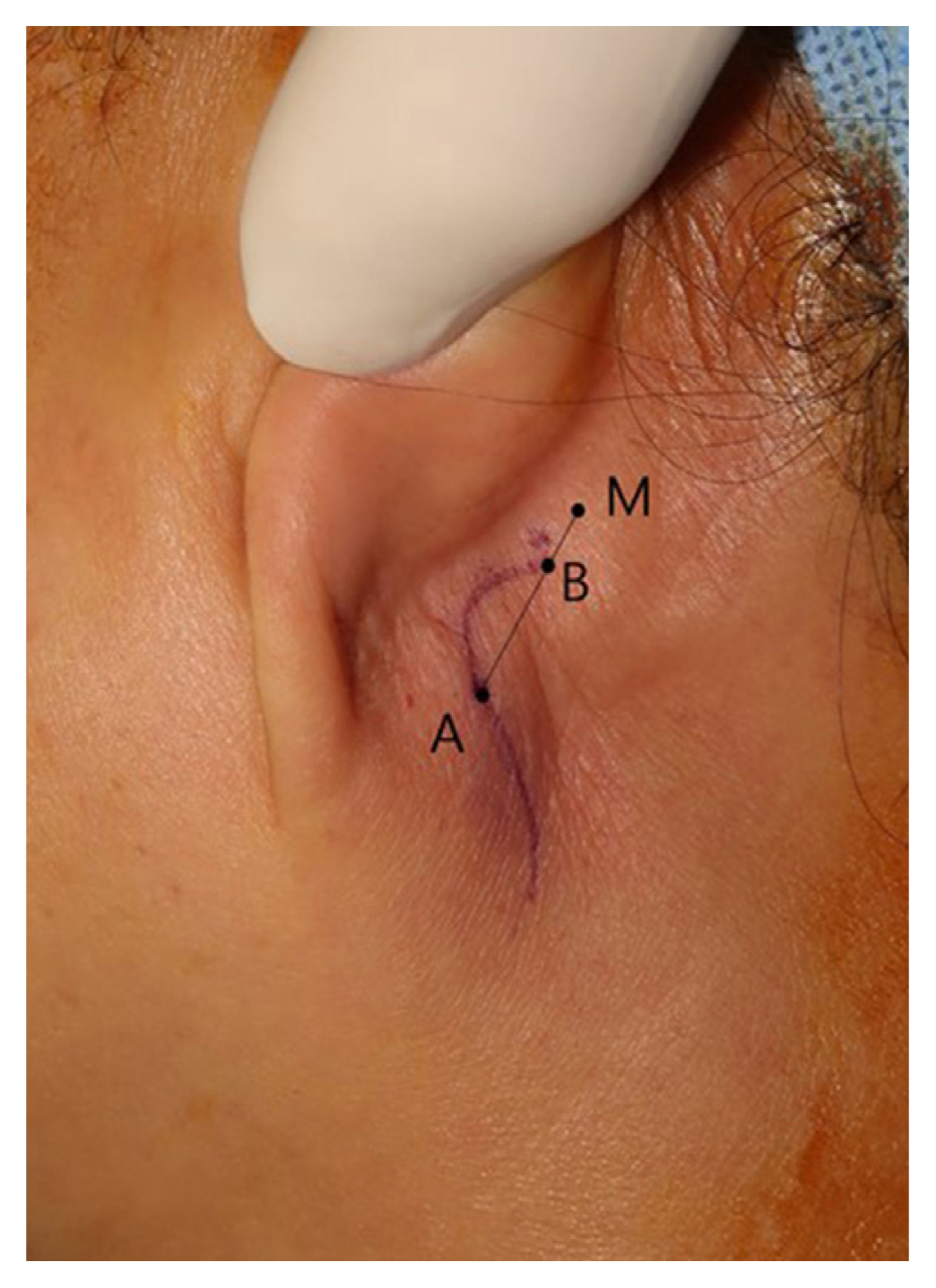
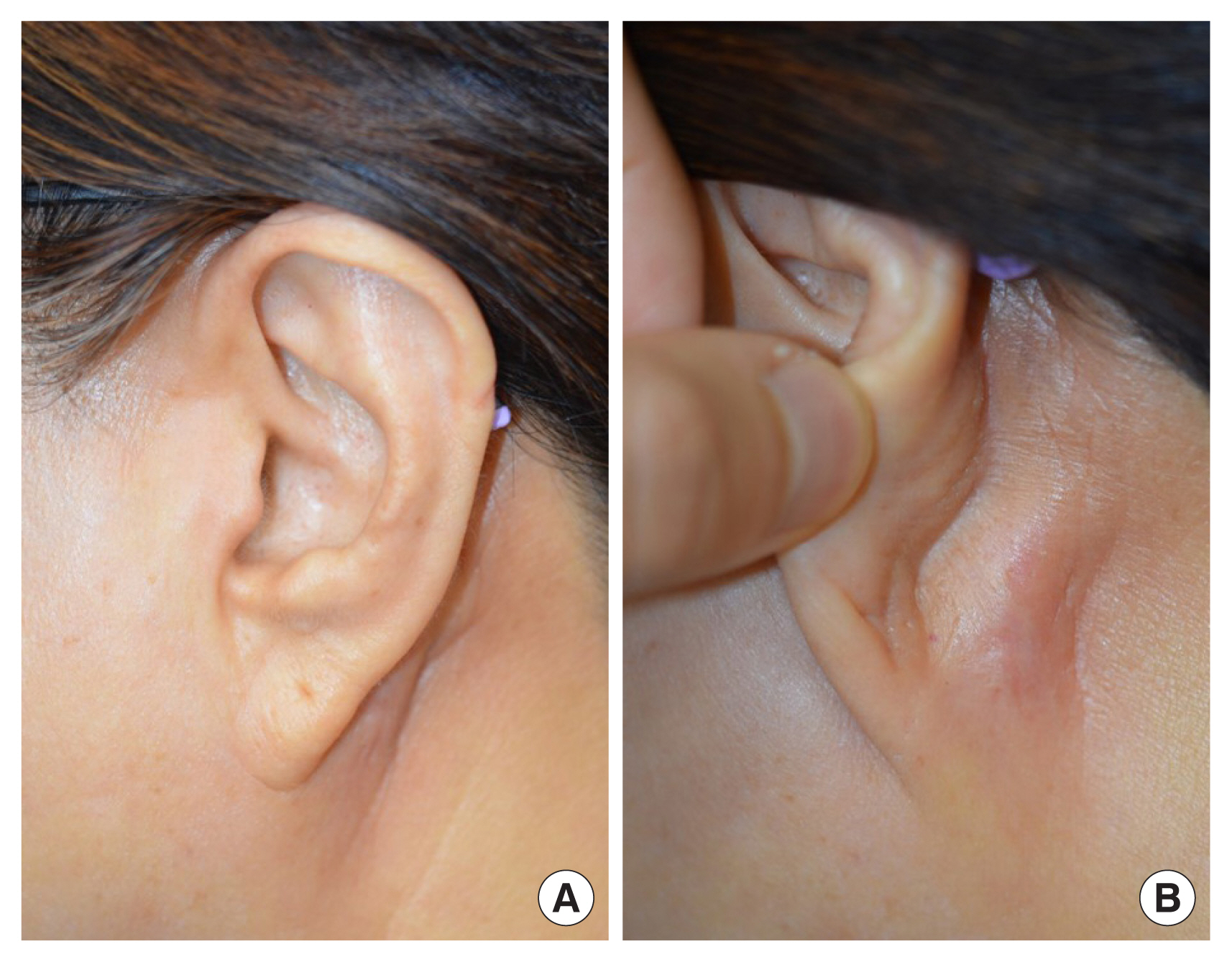
The present method is simple to design, easy to perform, and can be performed under local anesthesia. We observed a case of congenital pixie ears with tapered and low-set earlobes (Fig. 1). The patient was a 64-year-old woman who had congenital bilateral pixie ears and was dissatisfied with her appearance. Pixie ear was hereditary, and her two sisters also had it. She has always wanted to take correction on it. The procedure required only elevation of the skin and trimming of the redundant skin. The incision was planned in the retroauricular region; we took the position 1 cm posterior to the midpoint of the earlobe as point A, and the center of the mastoid process as point M. In the line connecting points A and M, point B, which is close to point M by 2:8, was determined as the suture point because of tension on around skin (Fig. 2). After the skin was incised along the design, the neck skin on infraauricular area was undermined in subcutaneous layer and elevated for redraping. Point A was approximated toward point B and sutured without tension. The remnant skin between point A and point B was trimmed (Fig. 3). The patient reported a satisfactory result after 3 years of surgery (Fig. 4).
DISCUSSION
The skin redraping method for correction of pixie ear is simple and easy to perform. The corrected earlobe shows a more natural appearance than the earlobe repositioned through conventional surgery. The scar appears only in the retroauricular region, so it is unnoticeable. Skin redraping avoids tension, which is another important factor contributing to scar minimization.
Pixie ear is a noticeable deformity [1], but it has not received as much attention as microtia, anotia, prominent ear, or traumatic ear [2,9,10]. Pixie ear has an attached, tapered, and low-set earlobe and can be congenital or acquired [1ŌĆō4]. Acquired factors include trauma, rhytidectomy, and total reconstruction of ear, among which rhytidectomy results in excessive skin resection around the ear or insufficient suspension of the deep soft tissues [1,11].
Traditional methods for pixie ear have been described. Most of the methods excise the caudal portion of the lobule and reattach it in a more superior position [5,6]. Such methods, however, result in smaller earlobes [7], or the scar along the border of the earlobe disturbs the earŌĆÖs natural appearance and can become hypertrophied [6]. In addition, correction of pixie earlobe is combined with dermofat graft to increase the volume of the earlobe [7].
The concept of the present method is modified from medial epicanthoplasty using the skin redraping method [8]. Skin redraping epicanthoplasty removes the hood of the epicanthal fold and widens the medial canthus. Likewise, skin redraping correction of pixie ear removes the hood of the pixie earlobe and shapes the intertragal notch between the earlobe and the jaw line.
In this method, the scar sits in the retroauricular area and is inconspicuous when viewed from the front. Finally, skin redraping for pixie ear creates a natural appearance with tension-free and invisible scars in the retroauricular region.
The skin redraping method for correction of pixie ear is simple and easy and creates a natural appearance with tension-free and invisible scars in the retroauricular region.