INTRODUCTION
Fibrin glue is widely used for hemostasis, wound healing, and tissue adhesion in several surgical fields, including skin grafting, microvascular surgery, breast surgery, neurosurgery, facelift surgery, and cardiac surgery. It can also be used for implant fixation in orbital wall fracture surgery [1,2]. Fibrin glue itself is considered very safe in terms of complications, although viral transmission may theoretically occur. Nonetheless, complications can take place when fibrin glue is used inappropriately [3,4]. Herein, we report an uncommon postoperative complication caused by the inappropriate application of fibrin glue in orbital wall fracture surgery.
CASE REPORT
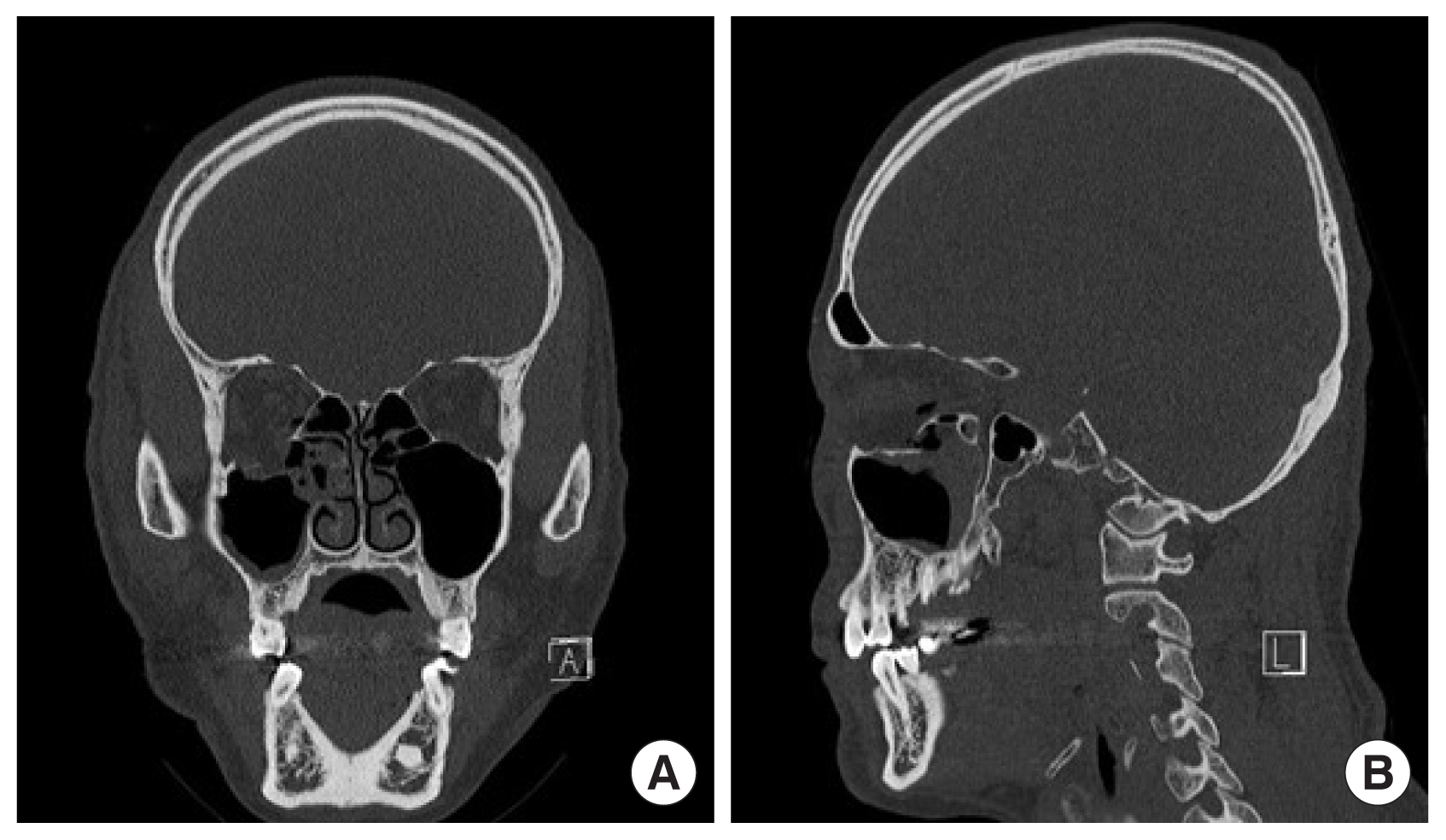
A 65-year-old man with no significant medical history presented to the emergency department with periorbital swelling and tenderness, with an open wound on the right infraorbital area caused by trauma. A clinical examination revealed double vision and limited eyeball movement on upward gaze. A 5-cm-long subcutaneous layer laceration was also noted. Computed tomography (CT) images revealed a right orbital floor fracture reaching the posterior region, with herniation of soft tissues in the maxillary sinus (Fig. 1).
The open wound in the right infraorbital area was sutured under local anesthesia. Five days after admission, surgical repair of the fracture was performed through the previously sutured wound under general anesthesia. After reduction of the herniated tissues, an absorbable implant (T&R Mesh - orbital type; T&R Biofab Co., Ltd., Siheung, Korea) was trimmed to be slightly larger than the defect and inserted. A forced duction test after implant placement showed a negative result, and globe motility was intact. Next, 1.5 cc of fibrin glue (Greenplast-Q, Green Cross Co., Yongin, Korea) was applied between the implant and the orbital tissues for implant stabilization, hemostasis, and wound healing. The fibrin glue was applied without difficulty, and there was little bleeding in the operation field. After the initial operation, there were no specific ocular symptoms and pain; however, we noted mild swelling, diplopia, and a slight limitation of eyeball movement. We considered these to be temporary postoperative sequelae and prescribed a corticosteroid to decrease the swelling. Nonetheless, the patient complained of persistent diplopia and limited eyeball movement.
Therefore, a postoperative CT scan was taken 4 days after surgery. The CT scan showed a well-defined, homogeneous, mass-like lesion just under the extraocular muscle. The herniated tissues were well reduced, and there was no evidence of hematoma formation. Magnetic resonance imaging (MRI) was thus performed 5 days after surgery for an accurate diagnosis of the lesion. Similar to the CT scan, a mass-like lesion was observed on MRI. According to the radiologist, there was a focal non-enhancing mass-like lesion. The mass was ovoid and measured about 1.5Ă0.6Ă1.2 cm. The radiologist thought it was a foreign body, but stated that, although unlikely, it could be a hematoma (Fig. 2).
We planned a second operation, which was performed under general anesthesia 6 days after the first surgery. Restriction was noted in the forced duction test. We approached the surgical site through the previous suture. During exploration, a clot formed by the previously applied fibrin was observed between the implant and soft tissues. It was thick in the vertical dimension and narrow laterally, since it was pooled on the concave implant without sufficiently covering the implant (Fig. 3). The fibrin clot also interfered with the movement of the muscle by compression in a confined area. Since there were no adhesions, it was removed easily, and the forced duction test was negative in an intraoperative examination (Fig. 4).
Next, 1.5 cc of fibrin glue was applied again carefully to stabilize the implant. We performed the forced duction test again as a final check. After the second operation, the patientâs symptoms were relieved and he was discharged without additional complications.
DISCUSSION
As a topical agent, fibrin glue is constituted using two separate syringes; when mixed, it forms a stable, semi-solid fibrin clot by a reaction similar to the last step in the coagulation phase of physiologic hemostasis. Its efficacy has been thoroughly documented in the literature. Therefore, many surgeons have used fibrin glue as a hemostatic agent, a sealing agent, an adhesive agent, and, recently, as a targeted delivery system [1]. Fibrin glue has been used as an adjunct in many surgical specialties, including cardiothoracic surgery, neurologic surgery, skin grafts, facelift surgery, breast surgery, gastrointestinal surgery, and microvascular surgery. It has also been used for facial bone surgery [2,5,6].
The orbital wall is thinner and more fragile than other bones, and the decision to perform surgical repair is determined by the patientâs condition and severity [7]. A bone defect may occur if repositioning the fracture fragment does not achieve sufficient stabilization and fracture fragments are displaced from the orbital cavity. Surgeons usually reconstruct bone defects using implants, and proper implant fixation is essential to prevent implant displacement. In a blow-out fracture that does not need an implant, rigid fixation of the bone segments is important [8,9]. Wire, screws, and plates are usually used for fixation of the implant or bone fragments. However, it is sometimes difficult to make holes in the remaining bone and fix them firmly. Using fibrin glue can overcome this problem. Therefore, we routinely use fibrin glue for implant fixation in orbital wall fracture surgery [10â14].
Although viral transmission may theoretically occur as a complication of fibrin glue, its manufacturing process is strictly regulated; as a result, there have been no known cases of viral transmission associated with the use of commercial fibrin glue. Fibrin glue is only contraindicated in patients with hypersensitivity to bovine proteins due to the presence of bovine aprotinin [3]. Nonetheless, several studies have reported that the inappropriate application of fibrin glue can cause complications. Grossman et al. [4] observed complications while using fibrin glue as an alternative to reduce the use of bulky dressings, drains, and postoperative garments in aesthetic facial procedures. In their study, 105 patients underwent 128 operations, and there were 10 cases of seroma and five cases of skin necrosis in the early postoperative period. The authors found that problems occurred in various aspects of the preparation and application of fibrin glue (e.g., poor melting, inappropriate positioning, inconsistent application, and incorrect application timing) rather than in the fibrin glue itself. As a relevant parallel to the present study, nonhomogeneous application and exceptionally thick areas of fibrin glue caused problems by acting as a barrier. They also stated that no more complications occurred after they recognized and fixed this problem [4]. Similarly, OâGrady et al. [5] stated that a thick layer of fibrin glue between the graft and host bed interface interfered with the healing process to a greater extent than a thin layer of fibrin glue in a skin graft, potentially resulting in graft failure. Ohta et al. [15] also performed transposition surgery in vessels with adhesion and recommended that the smallest possible amount of fibrin glue should be used to avoid adhesion to surrounding neurovascular elements. However, no previous reports have described fibrin glue complications in blow-out fracture surgery, as described herein.
In facial bone surgery, it is important to apply fibrin glue sufficiently and homogeneously, but not thickly. There are no guidelines on the dosage and technique for using fibrin glue in blow-out fracture surgery. However, based on our experience, the application of 1.0 to 1.5 cc of fibrin glue, mainly on the implant margin, is adequate depending on the size of the defect and implant. We have used this method for many years, and until this case, we obtained satisfactory results without complications. In this case, we did not apply the fibrin glue with sufficient care, which is thought to have been the cause of the complication. When fibrin glue is used for hemostasis or wound healing in other parts of the body, inappropriate application would be unlikely to cause a complication, and even if a complication does occur, the fibrin glue will be absorbed over time. However, the infraorbital cavity has unique anatomical features. This confined and concave space includes small but important muscles responsible for fine movements of the orbit. As a result, inappropriately applied fibrin glue can form a thick fibrin clot in this confined space and compress the tissues and muscles, thereby restricting ocular muscle movement. The movement of the eyeball is very important in daily activities, and even a slight limitation can cause severe discomfort.
In our case, it might have been possible for the symptoms to be relieved as the fibrin glue was re-absorbed over time. However, we did not initially know that the fibrin glue was the cause of the complication. Therefore, we planned exploratory surgery to remove the unknown mass shown on imaging, which was thought to be the cause of the patientâs symptoms.
In conclusion, careful attention and precisely controlled placement are required during blow-out fracture surgery using fibrin glue. Even if the surgical field of view is narrow, we must visually check whether fibrin glue is applied properly to the desired area with a homogeneous thickness, and a spray applicator can help for this purpose [16]. After application, tissue traction should be maintained until clot formation. An additional forced duction test after clot formation is very helpful as a final check. Finally, application of a large volume of fibrin glue should be avoided.