INTRODUCTION
The orbital wall is one of the most commonly involved sites for facial bone fractures followed by the nasal bone and mandible. The orbital floor is particularly susceptible to fractures because of its exposed position and thin concave bones. Furthermore, sequelae of untreated orbital floor fractures include diplopia, enophthalmos, extraocular muscle dysfunction, and infraorbital nerve anesthesia [1]. Although patients cannot recognize such symptoms, the indications for surgical management include radiographic evidence of extensive fracture or displacement of soft tissue. Some orbital floor fractures require only observation. However, surgical reduction should be considered when enophthalmos is expected due to an orbital volume change, soft tissue herniation or entrapment of extraocular muscles. Furthermore, reducing an orbital fracture is rather unique, as is it primarily completed with an implant, not bone fixation.
An implant is used to span the orbital floor defect to prevent tissue reherniation. Many autogenous and alloplastic materials have been used, including silicone, methylmethacrylate, Teflon, Gelfilm, bone, cartilage, and others. Most plastic surgeons tend to use alloplastic implants to repair orbital floor fractures, whereas others use autogenous grafts. However, autogenous grafts have various disadvantages such as graft absorption, donor site morbidity, and the need to harvest. Complications associated with alloplastic implants are rare with a prevalence of 0.4% [2]. Various types of complications, such as infection, abscess, lacrimal duct obstruction and exposed implants have been reported.
We present a patient who developed a late periorbital hematoma 8 months after reconstruction of the orbital floor with a Medpor (porous polyethylene) implant. A late complication after inserting an alloplastic implant has rarely been reported in Korea. In particular, orbital hemorrhage surrounding the implant is a rare complication of an alloplastic implant, as seen from a few case series.
CASE REPORT
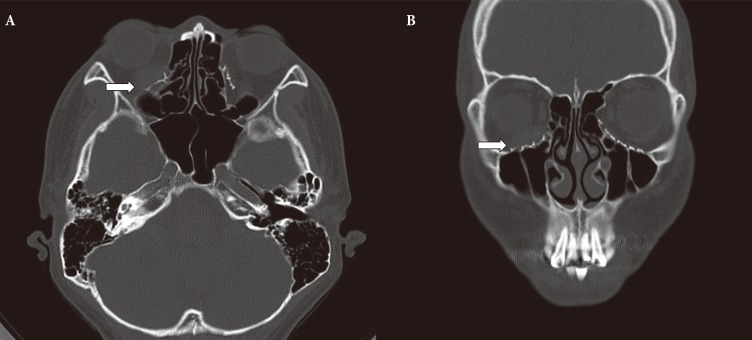
A 20-year-old male had blowout fractures of bilateral orbital floors that were reconstructed with Medpor implants 8 months prior at our institution (Fig. 1). The patient represented to our clinic because of gradual protusion of the right eye, which had started 4 days earlier without any additional trauma history since the initial operation. He had diplopia and restricted ocular motility on primary or down gaze, without headache. Exophthalmos was determined by a Hertel exophthalmometer with a relative protrusion of 20 mm for the right eye. The patient also had scleral show and vertical dystopia with the right eye being approximately 3 mm higher than the left. CT scan revealed a subperiosteal mass around the orbital floor implant. The right inferior rectus muscle was displaced 0.7 cm superiorly. The size of the mass was 2.3×2.0×1.0 cm (Fig. 2).
The patient underwent exploration via a subciliary incision through the previous scar. A fibrous capsule was surrounding the mass presumed to be hematoma. The fibrous capsule was dissected and partially removed because of the adhesions to the surrounding orbital structure and implant. A dark brown hematoma was identified and evacuated from the subperiosteal plane above the previously inserted Medpor implant, which was removed during this operation (Fig. 3). The patient did not wish to remove the implant in the contralateral orbit. Postoperatively, the ptoptosis was fully resolved. At one week, the remaining symptoms improved significantly by one week without diplopia or visual disturbance. No complications, such as pain, ocular muscle restriction, recurrence of hematoma, or bleeding were noted during the 11-month follow-up period.
DISCUSSION
Alloplastic implants have been used for orbital bone fractures and are generally well tolerated. Various implants have been used to reconstruct the orbital floor and prevent soft tissue herniation. In particular, Medpor is a non-absorbable implant material with high flexibility, and has a multiporous structure and the ability to form vasculature toward adjacent tissues. Medpor provides structural support, is well tolerated by surrounding tissue, and has a low risk of exposure and infection [2]. Various complications associated with alloplastic implants have been reported but are rare and found in isolated case series. A thick or malpositioned implant can induce superior or anterior displacement of the eyeball. If dead space is present between the implant and the orbital floor, fluid can easily collect, and the implant becomes very susceptible to infection. Due to its proximity to the maxillary sinus, the orbital floor fracture is exposed to risk of infection. Implants with smooth surfaces, such as silicone or Teflon, form a capsule around the defect in many cases, and vessels cannot easily penetrate the implant. This allows bacteria to colonize more easily around the implant. However, venous perforating branches from the orbital floor penetrate into the multiporous structure of Medpor. Thus, Medpor has a relatively low risk of bacterial infection but has a risk of bleeding or hematoma formation [3,4].
Many studies have analyzed the relationship between alloplastic implants and complications after orbital wall surgery. Common complications are proptosis, hyperglobus, inferior scleral show, orbital discomfort, diplopia, and motility restrictions. A few cases had clinical evidence of optic nerve compression. In a review of 583 orbital floor reconstructions with Medpor, Lee et al. [1] reported postoperative hematomas in only four patients (0.7%). An implant can cause low-grade irritation with evidence of chronic inflammation and form a fibrous capsule around the irritation. Gilhotra et al. [5] reported two cases of orbital hemorrhage 3 months after alloplastic orbital implant and estimated that capillaries in the capsule surrounding alloplastic implants were the main source of orbital hemorrhages in such cases. This hypothesis was further supported by Mauriello et al. [6] who studied implant capsules removed from patients with delayed hemorrhage after orbital floor reconstruction.
Dufresne et al. [7] suggested that periorbital bleeding usually originates from branches of the infraorbital artery or the penetrating venous branches in the orbital floor. In our case, the hemorrhage presented as a large cystic subperiosteal mass over the orbital floor implant. We presumed the mass to represent infected implant or hemorrhagic cyst; however, no evidence of abscess or a foreign body reaction was detected. We speculate that the etiology was rupture of capillaries growing within the implant pseudocapsule. Several authors have reported cases of late complications after alloplastic implant surgery and onset varied from weeks to years. Such hemorrhages have occurred with various implants and do not appear to be common with one particular implant type [1].
The origin or exact cause of a late hemorrhage is unclear and controversial. However, many capillaries may be present within the capsule around the implant; they can be ruptured and induce severe hemorrhage or hematoma even several years later. If the implant remains and compresses the orbital space, visual activity may be compromised and orbital rim discomfort will not resolve. Thus, the implant should be removed and re-evaluated as soon as possible. If hematoma is simply drained without removal of the implant, hemorrhage may reoccur due to rupture of a thin-walled vessel in the capsule [7]. It is difficult to accurately diagnose hemorrhage secondary to an orbital floor implant failure because of incomplete follow up and rarity of presentation and because of difficulties in the differential diagnosis between a benign cyst and hemorrhage. This report suggests that orbital hemorrhage following alloplastic orbital floor implantation may present with a variety of symptoms that may be slow in onset and even occur many years after the original repair.