Cleft lip and palate surgery during COVID-19 pandemic in Indonesia: a 36-month experience at the Bandung Cleft Lip and Palate Center
Article information

Abstract
Background
In Indonesia, the prevalence of cleft lip and palate increased from 0.08% to 0.12% between 2013 and 2018. Children with cleft deformities typically undergo staged surgery. However, the coronavirus disease 2019 (COVID-19) pandemic has had negative impacts on the healthcare sector, including the suspension of elective procedures; this has raised concerns about the safety of performing surgery and the functional consequences of delaying treatment, the latter of which is associated with poor prognosis. The purpose of this study was to report the characteristics of clefts treated by the Bandung Cleft Lip and Palate Center team during the pandemic period.
Methods
This brief comparative study based on a chart review was conducted at the Bandung Cleft Lip and Palate Center. We statistically evaluated data from all patients treated between September 2018 and August 2021. Frequency analysis was performed to analyze the average number of each procedure by age before and during the COVID-19 pandemic.
Results
Data from 18-month periods before (n = 460) and during (n = 423) the pandemic were compared. Cheiloplasty procedures were examined (pre-pandemic, n = 230; pandemic, n = 248); before the pandemic, 86.1% were performed according to the treatment protocol (patient < 1 year old), and this proportion non-significantly dropped to 80.6% during the pandemic (<i>p</i> = 0.904). Palatoplasty procedures were also compared (pre-pandemic, n = 160; pandemic, n = 139); the treatment protocol (patient 0.5–2 years old) was followed for 65.5% of procedures before the pandemic and 75.5% during the pandemic (<i>p</i> = 0.509). Additionally, 70 (mean age, 7.94 years) revision and other procedures were performed before the pandemic and 36 (mean age, 8.52 years) during the pandemic.
Conclusion
The cleft procedures performed at the Bandung Cleft Lip and Palate Center did not significantly change during the COVID-19 pandemic.
INTRODUCTION
Cleft lip and palate represent the most common congenital facial abnormalities globally. According to the World Health Organization, the incidence of cleft lip and palate is 15.37 per 10,000 live births [1]. Numerous factors contribute to the development of cleft lip and palate, including genetic predispositions, folic acid deficiency, smoking, alcohol consumption, obesity, stress, low zinc levels, fever during pregnancy, use of topiramate medications, race, geographic conditions, and socioeconomic factors [2-6].
In Indonesia, based on the Basic Health Research (Riset Kesehatan Dasar/RISKESDAS) studies, the national prevalence rate of cleft lip and palate increased from 0.08% to 0.12% between 2013 and 2018. The National Guidelines for Medical Services, which address the management of cleft lip and palate, indicate that the national prevalence of cleft lip in Indonesia is 0.2%. The annual incidence of cleft lip and palate in Indonesia is 7,500 cases [7].
Children with this cleft deformity undergo various stages of treatment and surgery, which can lead to developmental and growth challenges. Comprehensive team-based management is essential for successful patient care, which requires a team of specialist doctors from various fields, including craniofacial plastic surgery, pediatrics, anesthesiology, otolaryngology, medical rehabilitation, psychiatry, speech therapy, nursing, orthodontics, prosthodontics, and social work. Ideally, the treatment protocol for cleft lip and palate patients should be designed to achieve proper occlusion, normal speech function, and a natural appearance, while minimizing the risk of complications [8].
The coronavirus disease 2019 (COVID-19) pandemic has had a detrimental effect on all aspects of life, particularly healthcare. Patients with various medical conditions have experienced treatment delays, including the postponement of elective procedures. Cleft lip and palate are common congenital diseases that necessitate early interdisciplinary care; however, uncertainty surrounds the safety of conducting surgery during the COVID-19 pandemic and the functional consequences of postponing treatment. Delays in surgery are linked to a worse prognosis, and the heightened morbidity and mortality cannot be overlooked [9].
Resources are currently being focused on developing testing, ensuring adequate supply chains of personal protective equipment and ventilators, and implementing lockdown measures to prevent disease spread. As of the time of writing, many countries have mandated the cancellation of all surgical operations, except for emergency and cancer-related procedures, with the goals of preserving the health of healthcare workers, reducing the strain on personal protective equipment procurement, freeing up operating room space for use as so-called “surge” intensive care units, and preventing virus transmission to surgical patients. In most low and middle-income countries, elective surgery has been halted due to nationwide lockdowns aimed at stopping the spread of infection. Hospital services and travel have come to a standstill, and restrictions on patient movement have made accessing hospitals difficult [10].
Postponing surgery for cleft lip and palate exacerbates the psychological, nutritional, and speech difficulties experienced by patients and their families. In a recent publication, a consensus among providers indicated that cleft lip surgery could be delayed for up to 3 months without adverse effects on patients. However, with the duration of the pandemic now exceeding 12 months, deferred surgery may fall outside this recommended timeframe [10]. Regulations vary across countries, but fear of contracting COVID-19 and concerns about surgical and postsurgical complications in infected patients have contributed to delays in resuming elective procedures. For example, in India and Ghana, elective surgery was suspended in all public hospitals, although most cleft surgical procedures in Ghana are performed in well-equipped public facilities [10].
METHODS
A brief comparative study based on a chart review at a single center was conducted at the Bandung Cleft Lip and Palate Center in Bandung, Indonesia over a period of 36 months (September 2018 to August 2021). To evaluate the impact of the pandemic, we divided the study period into the pre-COVID-19 era (September 2018 to February 2020) and the COVID-19 era (March 2020 to August 2021), as new COVID-19-related regulations were implemented in Indonesia starting in February 2020. Data were obtained from patient medical records, with all records from the study period included except for those with incomplete medical information. The statistical analyses were performed using SPSS version 26 (IBM Corp.). Frequency analysis was performed to analyze the average number of each procedure by age before and during the COVID-19 pandemic. The study was conducted in accordance with the principles of the Declaration of Helsinki, and written informed consent for the publication of clinical details and images was obtained from patients’ guardians.
RESULTS
Over the 36-month period, a total of 478 primary cheiloplasty procedures were performed. Of these, 230 (48.1%) took place in the pre-COVID-19 era, and 248 (51.9%) were conducted during the COVID-19 era. The most common age group for patients in both the pre-COVID-19 and COVID-19 groups was up to 6 months old (n = 146 [63.5%] vs. n = 143 [57.7%], respectively). No significant differences between eras were found in the age groups of the patients undergoing primary cheiloplasty (p = 0.904) (Table 1). The primary cheiloplasty procedure was considered appropriate for the patient’s age in the majority of cases for both groups (n = 198 [86.1%] and n = 200 [80.6%] in the pre-COVID-19 and COVID-19 groups, respectively). No significant differences between eras were found in the age-appropriateness of primary cheiloplasty (p = 0.070).

Comparison of patient age and age appropriateness for primary cheiloplasty procedures in the pre-COVID-19 and COVID-19 eras
A total of 299 primary palatoplasty procedures were performed. Of these, 160 (53.5%) were conducted in the pre-COVID-19 era, and 139 (46.5%) took place during the COVID-19 era. The most common age group for patients in both the pre-COVID-19 and COVID-19 groups was 12 to 24 months old (n= 99 [61.9%] vs. n= 98 [70.3%], respectively). No significant differences between eras were found in the age groups of the patients undergoing primary palatoplasty (p= 0.509) (Table 2). The primary palatoplasty procedure was considered appropriate for the patient’s age in the majority of cases for both groups (n = 105 [65.6%] in the pre-COVID-19 group vs. n = 105 [75.5%] in the COVID-19 group, respectively). No significant differences between eras were found in the age-appropriateness of primary palatoplasty (p = 0.323).

Comparison of patient age and age-appropriateness for palatoplasty procedures in the pre-COVID-19 and COVID-19 eras
During our study period, a total of 106 revision procedures were performed. Of these, 70 (66.0%) were conducted in the pre-COVID-19 era, and 36 (34.0%) took place in the COVID-19 era. We did not evaluate the appropriateness of the procedures by age, as various types of revision procedures were undertaken and each had different age recommendations. The mean age of the patients undergoing revision procedures was 7.94 years in the pre-COVID-19 era and 8.52 years in the COVID-19 era (p = 0.654) (Table 3).

Comparison of patient age and age appropriateness for other revision procedures in the pre-COVID-19 and COVID-19 eras
A month-by-month comparison was conducted by comparing the total number of procedures performed during the pre-COVID-19 era (September 2018 to February 2020) and the COVID-19 era (March 2020 to August 2021). The comparison was carried out in consecutive order, with the first month of the pre-COVID-19 era being September 2018 and the first month of the COVID-19 era being March 2020. Thus, the comparison of the first month for both groups was between September 2018 and March 2020. No procedures were performed during the second and third months of the COVID-19 era at our center due to the implementation of new COVID-19 regulations starting in March 2020 (Table 4, Fig. 1).

Month-by-month comparison of total procedures done at the Bandung Cleft Center during the pre-COVID-19 and COVID-19 eras
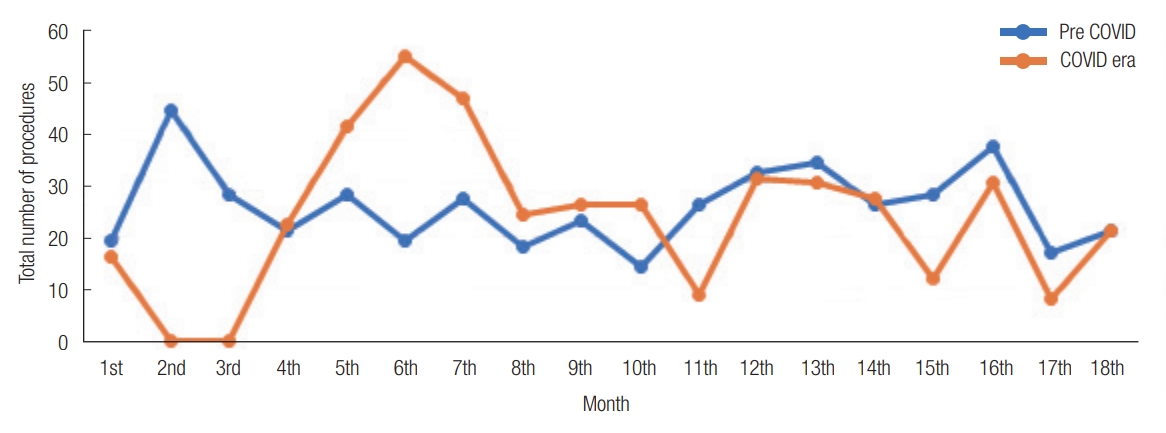
Month-by-month comparison of total procedures done at the Bandung Cleft Center during the pre-COVID-19 and COVID-19 eras. COVID-19, coronavirus disease 2019.
DISCUSSION
The first case of COVID-19 in Indonesia was documented on March 2, 2020. Following this, the government established a public health emergency regarding COVID-19 through Presidential Decree Number 11 of 2020. A large-scale social restriction (Pembatasan Sosial Berskala Besar, PSBB) policy was then stipulated through Government Regulation Number 21 of 2020 and Regulation of the Minister of Health Number 9 of 2020, which were applied to accelerate the management of COVID-19. These regulations not only governed public activity but also affected the operation of health services. Separate rooms and zones were recommended, work shift schedules were created, and elective procedures were halted due to the countrywide lockdown aimed at stopping the spread of infection. The PSBB policy impacted hospital services and travel, which came to a standstill, making it difficult for patients to access hospitals due to restrictions on movement. Essential health services (including family health and family planning services; the management of tuberculosis, human immunodeficiency virus, infectious diseases [such as leprosy, dengue hemorrhagic fever, and malaria], chronic diseases like hypertension, diabetes mellitus, and cardiovascular issues; mental health; immunization; critical inpatient therapy; emergency health conditions; and the treatment of general acute illnesses) were prioritized, with limitations on face-to-face health services [11,12].
At our cleft center, elective procedures were restricted, and patients underwent COVID-19 screening using polymerase chain reaction swabs prior to elective surgery. A positive result necessitated the postponement of the procedure and the quarantine of the patient. Travel across city borders was limited due to security and screening measures at checkpoints. New public and hospital regulations, as well as the emergency situation, substantially impacted our operations during the second and third months of the COVID-19 era, as no cleft procedures were performed for 2 months.
The safety of performing surgery during the COVID-19 pandemic and the functional impacts of delaying treatment must be considered, particularly for elective cases such as cleft procedures. American Cleft Palate-Craniofacial Association guidance recommends delaying primary cleft lip repair and prioritizing patient and provider safety when deciding whether to delay palate repair; however, the risk of postponing palate repair must be balanced against the risk of COVID-19 exposure for both the patient and the healthcare team [13,14]. At our center, the normal schedule for cleft surgery was resumed after only a 2-month delay in elective procedures, beginning in month 4 of the COVID-19 era. A total of 423 cleft operations were performed during the 18-month COVID-19 period, compared to 460 operations during the period prior to the pandemic. A month-by-month comparison revealed a varied number of procedures performed during the COVID-19 era, with an apparently greater fluctuation compared to the pre-pandemic period.
Regarding primary cheiloplasty procedures, no significant differences were observed in the number of procedures and the patient’s age group. Most patients were under 1 year old, which is the ideal age to undergo primary cheiloplasty. Similar findings were also observed for primary palatoplasty.
A study by Vander Burg et al. [10] demonstrated a 31% reduction in cleft procedures throughout 2020 compared to the previous year, 2019. Data from the World Bank Income Group revealed that all country groups experienced a significant decline in case rates from March to May 2020. A study conducted by Bruce et al. [15] indicated an increase in the mean age of patients and a delay in procedures during the pandemic period. In that study, the mean age at cleft lip and nose repair was 6.6 ± 1.9 months pre-pandemic (n = 23) and 8.0 ± 2.1 months in the pandemic cohort (n = 23) (p = 0.03). Six cleft lip and nose repairs during the pandemic period were rescheduled due to the ban on elective surgery, with a mean delay of 2.6 ± 1.8 months. The mean age at palatoplasty was 13.9 ± 2.2 months pre-pandemic (n = 26) and 14.1 ± 2.9 months in the pandemic cohort (n= 26) (p= 0.79). Seven palatoplasties during the pandemic period were delayed, with a mean delay of 3.3 ± 1.4 months [15].
In the present study, no significant differences were observed in the number of primary cheiloplasty and palatoplasty procedures, patient age groups, and age appropriateness of each procedure during the COVID-19 era compared to the pre-pandemic era.
Abbreviations
COVID-19
coronavirus disease 2019
PSBB
Pembatasan Sosial Berskala Besar
Notes
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Funding
None.
Ethical approval
The study was conducted in accordance with the principles of the Declaration of Helsinki. Written informed consent for the publication of clinical details and images was obtained from patients’ guardians.
Author contributions
Conceptualization: Ali Sundoro, Dany Hilmanto, Hardisiswo Soedjana. Data curation: Ali Sundoro, Dany Hilmanto. Formal analysis: Ali Sundoro, Dany Hilmanto, Hardisiswo Soedjana. Methodology: Ali Sundoro, Dany Hilmanto, Hardisiswo Soedjana, Ronny Lesmana. Project administration: Ronny Lesmana. Visualization: Dany Hilmanto. Writing - original draft: K Suryadinata. Writing - review & editing: Ali Sundoro. Investigation: Ali Sundoro, Hardisiswo Soedjana, Ronny Lesmana, K Suryadinata. Resources: K Suryadinata. Software: K Suryadinata. Supervision: Ali Sundoro, Dany Hilmanto, Hardisiswo Soedjana, Ronny Lesmana. Validation: Ali Sundoro, Dany Hilmanto, Hardisiswo Soedjana, Ronny Lesmana.
Acknowledgements
The authors would like to thank the staff of the Division of Plastic Reconstructive and Aesthetic Surgery, Department of Surgery, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia.