The cover of an ear thermometer probe as a split-thickness skin graft mold in external auditory canal reconstruction
Article information

Abstract
Maintaining the patency of the external auditory canal (EAC) during reconstruction is important because of its physiological role in hearing and immunological protective functions. The curved shape of the EAC presents a challenge when performing a skin graft. One of the key points for a successful skin graft is to ensure compression on the wound bed, and many novel methods, including prefabricated ear molds, have been reported for this purpose. In this study, we present a case of a skin graft performed to reconstruct a skin defect following excision of actinic keratosis in the EAC, using the cover of an ear thermometer probe as a mold for the graft to match the curvature of the EAC. This is an economical and practical method for secure compression dressing of a skin graft in the EAC.
INTRODUCTION
Deformities of the external ear canal (EAC) can be caused by tumors, burns, trauma, and malformations. Reconstruction is sometimes required after surgery of the EAC [1,2]. The patency and shape of the EAC must be maintained in order to preserve its functions, including hearing and protection against microbes [2]. Many surgical approaches with varying success rates for EAC reconstruction have been devised, including secondary healing, skin grafting, and a variety of local skin flaps [3].
Among these methods, skin grafting is commonly performed because of its technical simplicity. However, it has been associated with certain complications, including contracture formation, stenosis, and delayed wound healing [3,4]. Proper graft compression and shape maintenance have been suggested as ways to help overcome these shortcomings [5,6]. Many creative ideas have been described in the literature with the goal of providing proper structure and compression to difficult skin graft locations, including quilting sutures, negative-pressure wound therapy (NPWT), foam quilting, and surgical gloves [7-10]. In this report, we describe a case of EAC reconstruction with a skin graft after the resection of a premalignant lesion. The cover of an ear thermometer probe was successfully used as a mold to match the curvature of the EAC.
IDEA
A 55-year-old Asian woman presented to our clinic with a 1-week history of tinnitus in the left ear. The patient denied hearing loss, otalgia, otorrhea, bleeding, or vertigo. No visible lesions were observed in her outer ear. Otoscopy revealed a painless 1.0 × 1.5 cm patch-like lesion just above the tympanic membrane (Fig. 1). The left tympanic membrane was intact and no hearing impairment was observed on pure-tone audiometry. A further evaluation using computed tomography revealed no involvement of the temporal bone or head and neck structures.

Otoscopic findings of the lesion in a 55-year-old Asian woman with a 1-week history of tinnitus (left external auditory canal). A 1.0×1.5 cm, light-brown patch diagnosed as actinic keratosis is visible just above the tympanic membrane.
The lesion was diagnosed as actinic keratosis on skin biopsy. Due to the malignant potential of the lesion [11,12], local resection and reconstruction with a split-thickness skin graft (STSG) were planned. The EAC skin was surgically removed with partial cortical bone curettage to preserve the outer half of the EAC and the cranial portion. After resection, the skin defect size was 1.5 × 2.0 cm (Fig. 2). A 10/1,000-inch layer of skin was harvested with an air dermatome. To maintain the shape of the cone-shaped graft, a sterilized cover of an ear thermometer probe (MC-EP2 for ear thermometer model TH839S; Omron) was used as a mold for the EAC (part a in Fig. 3). This was used to bolster the skin graft on the EAC. In order to place the probe cover deeper, its rim was cut, and the body was punched with a 21-gauge needle to help drain the wound discharge. The harvested skin was placed on the tip of the probe cover and sutured using 5-0 coated Vicryl sutures (Ethicon Inc.) (part c in Fig. 3C). After positioning the skin, a mesh gauze was packed into the cavity of the probe cover and its opening was tagged with 4-0 black silk (AILEE Inc.) (part d in Fig. 3). The probe cover was subsequently placed in the defect using a bolster suture to hold the harvested skin in place and prevent skin graft displacement (Fig. 4). Both the graft dressing and thread gauze used for inner packing were changed every 3 days without disturbing the graft. Polyurethane foam dressing was used to treat the donor site. The wound had healed well without any complications at 2-week (Fig. 5A) and 3-month (Fig. 5B) postoperative follow-up visits.
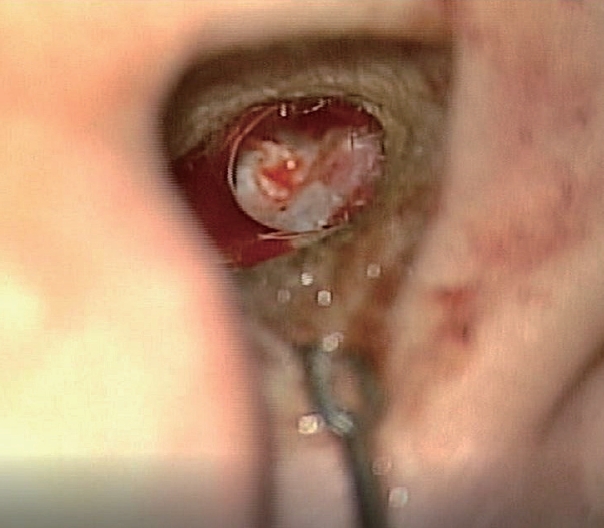
Microscopic view after resection of the lesion; the cranial portion of the external auditory canal was preserved. The final defect size was 1.5×2.0 cm with partial cortical bone resection.
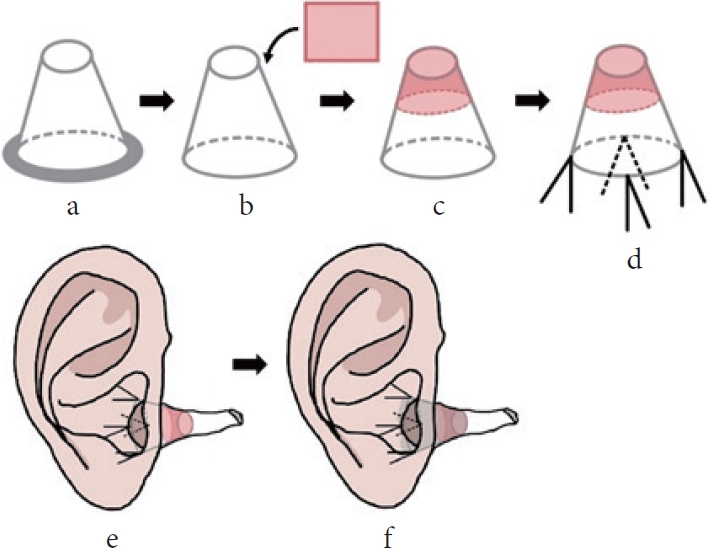
Schematic of the mold. (a) A cover of an ear thermometer probe was sterilized for surgery. (b) The rim of the probe cover was cut and a skin graft was placed over the cover. (c) The skin was fitted to the shape of the cover. (d) The probe was tagged with a silk suture. (e) The probe was pushed into the ear canal to place the skin graft over the defect. (f) Mesh gauze was packed into the probe cover for compression.

Immediate postoperative photograph of the patient; after fixing the probe cover at the auricle using black silk #4-0, a bolster suture was placed over the packing gauze.
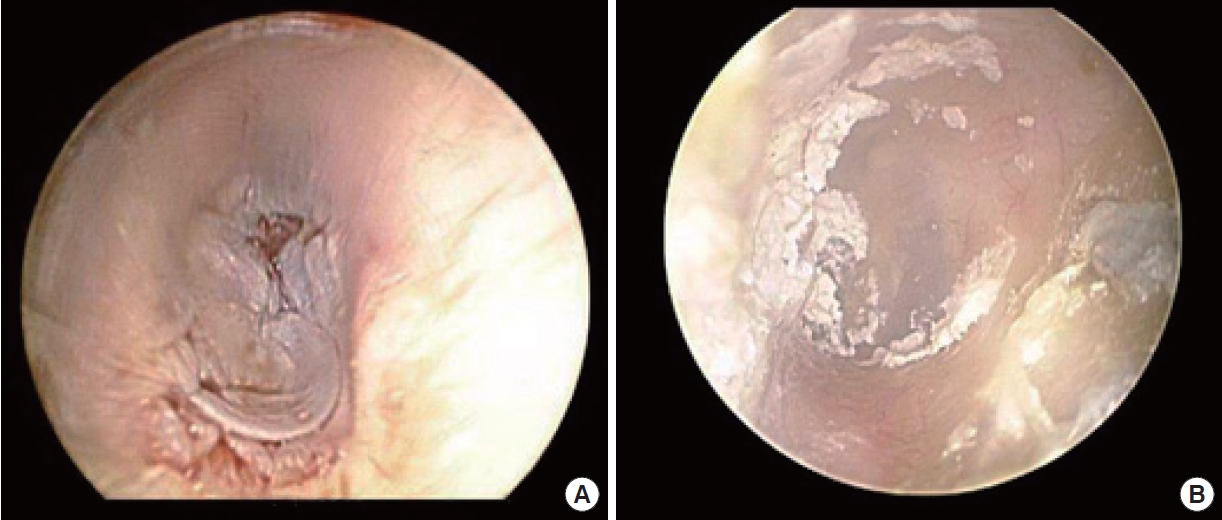
Photographs after surgery. (A) Skin graft 2 weeks after surgery. (B) Skin graft 3 months after surgery; the harvested graft was well-engrafted without any complications.
DISCUSSION
The maintenance of patency during EAC reconstruction is essential for the preservation of hearing function, continuity of access for routine ear cleansing, and physical examinations [2,4]. Various techniques are available for EAC reconstruction that help maintain its patency [3,4]. The three-dimensional curvature of the EAC makes it difficult to perform skin grafting; such curved surfaces require the optimization of techniques [13]. Defects smaller than 2.0 cm may be left to heal by secondary intention or adequately covered with a skin graft. To restore defects larger than 2.0 cm, local flaps and skin grafts may be used, as described in previous research [14]. In our case, a 2.0 × 1.5 cm defect resulted from the resection of actinic keratosis in the inner portion of the EAC. To minimize donor site morbidity and retain the shape of the canal, we reconstructed the defect using STSG.
Efforts were made to develop a suitable mold, because it is difficult to retain the harvested skin intact against the bony canal [5,6]. Although previous studies have proposed using a nasopharyngeal tube or ear mold stent [5,6], it is difficult to fit a nasopharyngeal tube to match the shape of the ear, and an ear mold stent requires a long manufacturing time. In addition, although ear molds can fit well, their usage period is rather short compared to the cost. NPWT and quilting sutures are also popular methods for skin graft dressing [8,10] that facilitate compression and drainage. They are, however, not appropriate for the narrow space of the EAC and the sensitive tympanic membrane.
Therefore, we used an ear thermometer probe cover as a mold for a skin graft in this case. As it was already made for the ear canal, only minimal additional trimming was required to make it suitable for this purpose. Furthermore, the probe cover facilitated serum imbibition and graft collection without causing canal stenosis or infection. Therefore, the use of a cover of an ear thermometer probe as a mold for an EAC skin graft has the potential to reduce costs and simplify surgery.
To achieve successful wound healing using a skin graft, it is important to maintain the grafted skin in close contact with the wound. Hence, a cover of an ear thermometer probe is a useful graft mold for EAC defect reconstruction using a skin graft.
Notes
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Funding
None.
Ethical approval
The study was approved by the Institutional Review Board of Seoul St. Mary’s Hospital (IRB No. KC20ZISI0865).
Patient consent
The patient provided written informed consent for the publication and use of her images.
Author contributions
Conceptualization: Kyoung Ho Park, Deuk Young Oh. Data curation: Chae Rim Lee, Sungyeon Yoon, Ji Hun Kim, Jangyoun Choi. Formal analysis: Jangyoun Choi. Methodology: Kyoung Ho Park, Deuk Young Oh. Project administration: Chae Rim Lee, Sungyeon Yoon, Ji Hun Kim, Jangyoun Choi, Kyoung Ho Park, Deuk Young Oh. Writing - original draft: Chae Rim Lee, Sungyeon Yoon, Ji Hun Kim. Writing - review & editing: Chae Rim Lee, Sungyeon Yoon, Ji Hun Kim. Supervision: Ji Hun Kim, Kyoung Ho Park, Deuk Young Oh.
Abbreviations
EAC
external ear canal
NPWT
negative-pressure wound therapy
STSG
split-thickness skin graft