Eccrine Poroma of the Postauricular Area
Article information
Abstract
Eccrine poroma is a common benign cutaneous tumor that originates in an intraepidermal eccrine duct. This tumor exhibits acral distribution (sole, palm), and is rarely encountered in the head and neck area. In fact eccrine poroma in the postauricular area has only been rarely reported. A 55-year-old female visited our hospital with a main complaint of a mass that first developed in the left postauricular area about a year previously. The mass was painless, soft, protruding, domed, and dark red in color, and had slowly enlarged (at presentation it measured 1×1 cm). Excisional biopsy was performed. Histological examination showed distinct features, and eccrine poroma was diagnosed. Follow-up at 6 months postoperatively showed no recurrence. The frequency of eccrine poroma is dependent on eccrine sweat glands density, and thus, usually occurs on the palms or soles. For eccrine poroma in the head and neck region, the differential diagnosis must rule out other masses, such as nevus, skin tag, pyogenic granuloma, cyst, basal cell carcinoma, and seborrheic keratosis. Importantly, 18% of poromas show malignant transformation, and can develop into porocarcinoma. For these reasons, an eccrine poroma in the facial area requires histological examination, complete excision, and follow-up.
INTRODUCTION
Eccrine poroma is a common benign cutaneous tumor that originates in an intraepidermal eccrine duct. This tumor mostly occurs in middle-aged or older adults, and is equally likely in both genders. Usually eccrine poroma exhibits acral distribution (sole, palm), and is rarely encountered in the head and neck area. In fact, eccrine poroma in the postauricular area has only been rarely reported [1]. We report a case of eccrine poroma in the postauricular area.
CASE REPORT
A 55-year-old female visited our hospital with a main complaint of a mass that first developed in the left postauricular area about a year previously. The mass was a solitary, asymptomatic, 1.0×1.0 cm sized, brownish, protruding, soft nodule with central dark crust (Fig. 1), and had slowly enlarged. There was no history of trauma or infection. Atypical nevus and pyogenic granuloma were considered as differential diagnoses, and an excisional biopsy was performed under local anesthesia.

Photograph showing a solitary, asymptomatic, 1.0×1.0 cm sized, brownish, protruding, soft nodule with central dark crust.
Histopathologic findings revealed that the tumor arose within the lower portion of the epidermis and extended downward into the dermis as broad anastomosing bands (Fig. 2A). Tumor cells had a uniform cuboidal appearance with a round basophilic nucleus (Fig. 2B). Follow-up at 6 months postoperatively showed no recurrence.
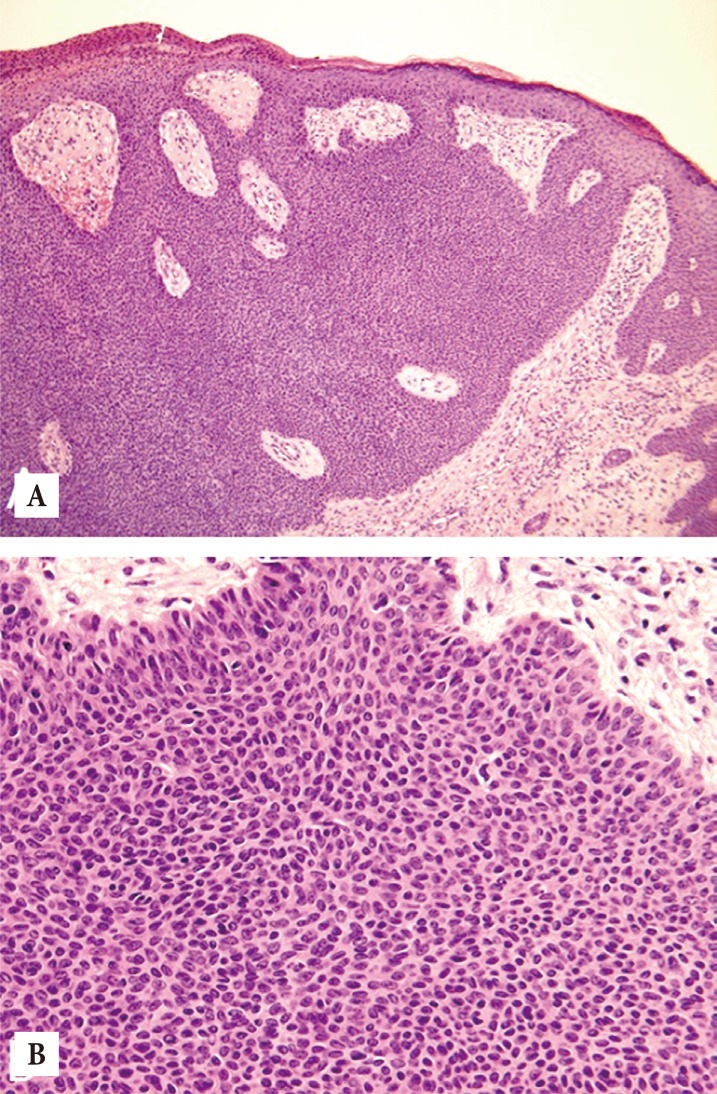
Microscopic findings. (A) The tumor arose within the lower portion of the epidermis and extended downward into the dermis as broad anastomosing bands (H&E, ×40). (B) Tumor cells had uniform cuboidal appearance with a round basophilic nucleus (H&E, ×200).
DISCUSSION
Eccrine poroma is a benign tumor that originates from the apical portion of an eccrine sweat gland. The frequency of eccrine poroma is dependent on eccrine sweat glands density, and thus, usually occurs on the palms or soles. However, eccrine poroma can develop in any part of the body with these glands [1].
Moore et al. [2] compared 10 cases of eccrine poroma in the head and neck with 10 cases with eccrine poroma in an extremity. They reported that eccrine poroma in the extremities was more likely to be pigmented, as was observed in the present case. Furthermore, they also reported that three cases of eccrine poroma in the extremities exhibited discharge and bleeding, caused pain, and showed a rapid growth pattern, whereas in our patient, eccrine poroma in the postauricular area did not display these symptoms.
Goldman et al. [3] reported that the most common location for eccrine poroma is the foot, followed by the hand (reported prevalences were 65% and 10%, respectively), and Hyman and Brownstein [4] reported 68% of eccrine poromas occur in feet, and that the remainder occur in various locations.
For eccrine poroma in the head and neck region, the differential diagnosis must rule out other masses, such as fibroma, nevus, skin tag, pyogenic granuloma, cyst, basal cell carcinoma, and seborrheic keratosis [12]. Importantly, Robson et al. [5] reported that 18% of eccrine porocarcinoma arised from benign eccrine poroma. For these reasons, an eccrine poroma in the facial area requires histological examination, complete excision, and follow-up.
Notes
No potential conflict of interest relevant to this article was reported.