INTRODUCTION
Primary cutaneous mucinous carcinoma (PCMC) is a rare low-grade malignant neoplasm derived from the eccrine glands [1]. These carcinomas most commonly arise in the head and neck region, with the eyelid being the most common site of origin [2]. It is slightly more common in men and appears most frequently between the ages of 50 and 70 years [3]. The prevalence is higher in white patients (77.2%) than in Asians (12.7%) or in African Americans (10.1%) [4]. We report a case of PCMC of the lower eyelid in a 51-year-old Asian male.
CASE REPORT
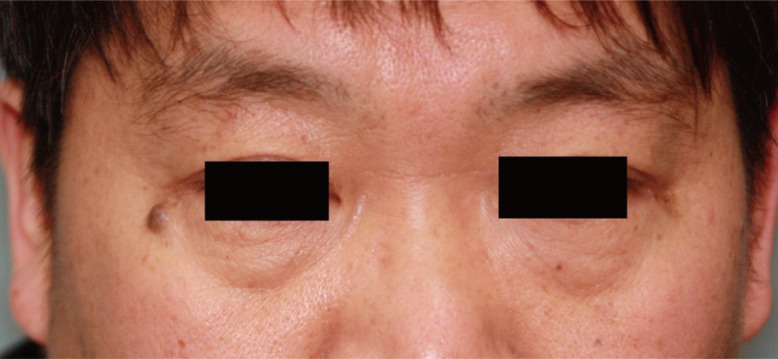
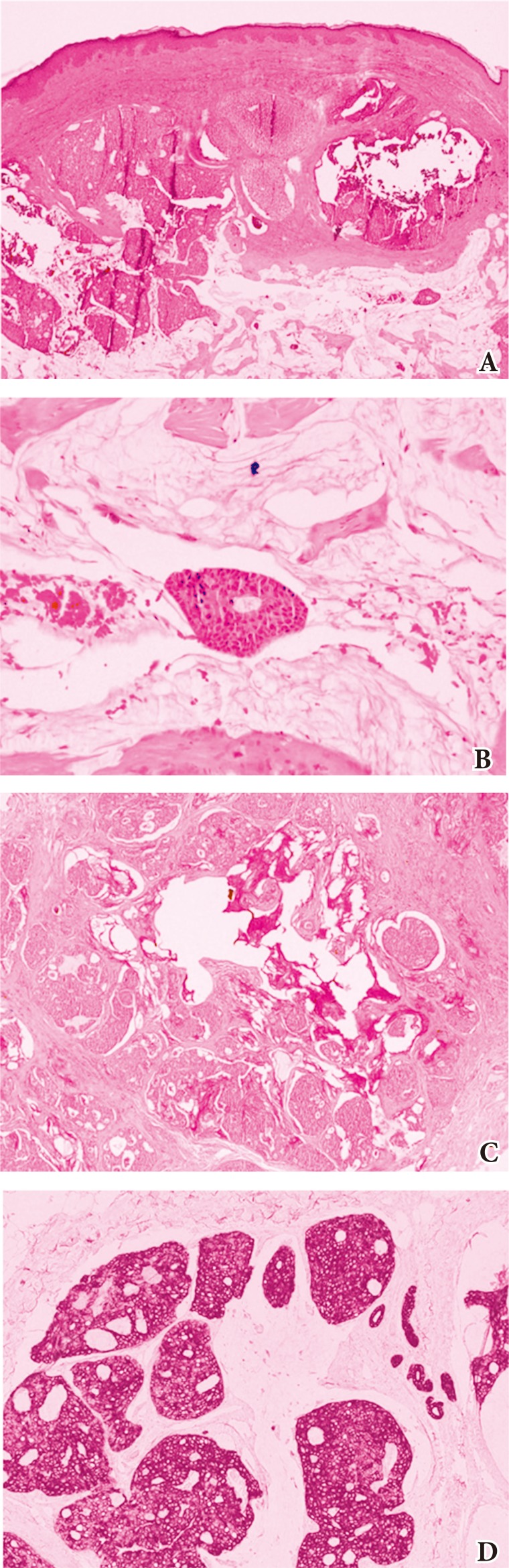
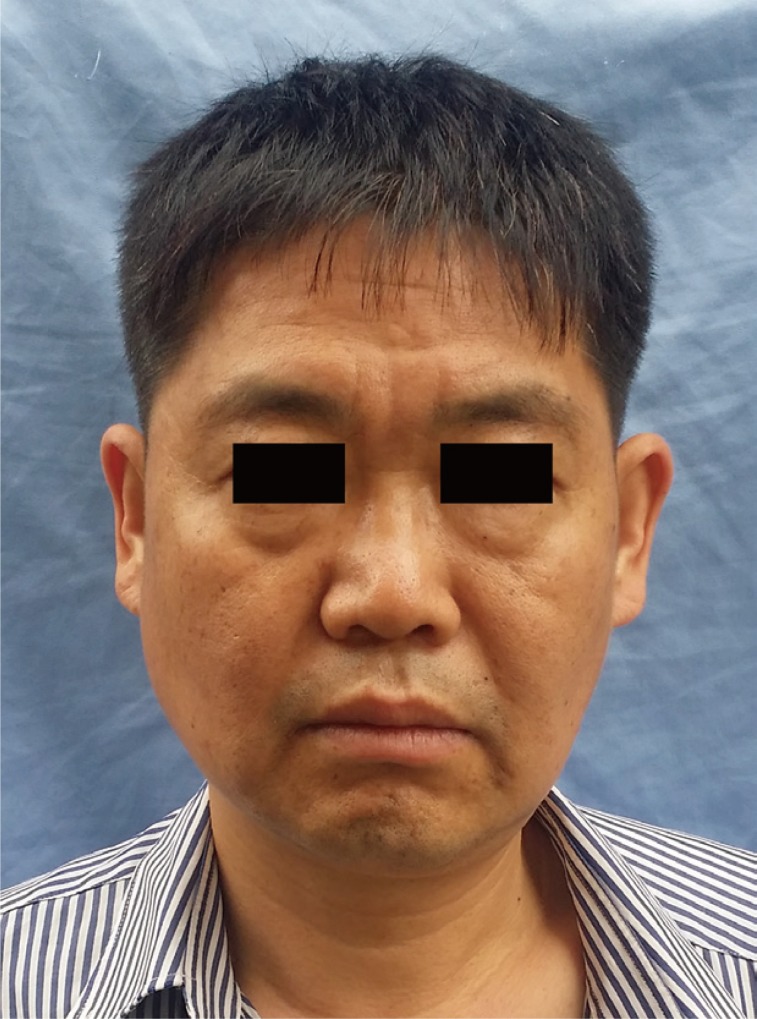
A 51-year-old male patient presented to the outpatient clinic with a painless nodule near the right lower eyelid. The mass had grown slowly over the past 3 years, and measured 0.9├Ś0.7 cm during examination (Fig. 1). The lesion appeared benign in clinical examination, and under local anesthesia, the patient underwent a 3-mm-margin elliptical excision and primary closure. Histologic study of this first specimen revealed epithelial cell islands floating in a mucin lake, with the final diagnosis being mucinous carcinoma. The epithelial component showed a solid and cribriform growth pattern and the tumor cells revealed moderate nuclear atypia and a mitotic aspect. Additional immunostaining study revealed that the tumor cells were immunopositive for cytokeratins (CK)-7 and negative for CK-20 with 10% Ki-67 positivity in the active area (Fig. 2). We performed re-excision of the surgical site with an additional 3-mm margin, which was free of malignant histology. The possibility of a metastatic primary mucinous carcinoma (e.g., breast or gastrointestinal tract) could not be completely ruled out, but a systemic evaluation by positron emission tomography-computed tomography revealed no other suspected site of malignancy. During a close follow-up over 2 years, the patient did not experience any postoperative complication or recurrence (Fig. 3).
DISCUSSION
PCMC was first described by Lennox et al. [1] and is a rare subtype of sweat gland tumor. Controversy about the apocrine or eccrine origins of this tumor has existed, but most authors favor eccrine differentiation as the origin [5]. The affected population tends to be older, in the range of 50 to 70 years [3,4]. Clinically, PCMCs have been characterized as slow-growing (with a duration of several months to several years), painless, 0.7ŌĆō2.5 cm in size, nodular, pigmented lesions that may be ulcerated, crusted or with telangiectasis [6,7,8]. The single most common site is the periorbital region (40%) and over half of those are lower eyelid lesions [2,9].
PCMC is a sharply circumscribed tumor in the dermis and subcutis with no connection to the epidermis [10]. Because of its location, PCMC must be differentiated from sebaceous gland and other sweat gland carcinomas, which have far less favorable prognoses, and also from basal cell carcinoma, keratoacanthoma, and nevi including vascular lesions such as Kaposi sarcoma [7,8,10]. Differentiation may be based on the expression pattern of CK. Eccrine mucinous carcinomas are CK-7 positive and CK-20 negative, unlike metastases of the gastrointestinal tract, which are CK-20 positive and CK-7 negative [11]. In addition, skin metastases normally contain atypical cells, exhibit increased mitotic activity, and are usually surrounded by collagen bundles [12].
Primary mucinous carcinoma of the skin has a relatively good prognosis with lower rates of distant metastases (9.6%, commonly to regional lymph nodes), but local recurrence rate is higher at 29.4% [6,13]. Since the 1979 study by Wright and Font [2], PCMC of the eyelid has been regarded as having high rates of recurrence (up to 40%). In a more recent study, in 2004, Marra et al. [14] reported a recurrence rate of 34% in the eyelid.
PCMC is resistant to chemotherapy and radiotherapy [15]. The treatment recommendation has been surgical excision with a minimum of 10-mm margin [6,16,17]. Morbidity from PCMC of the eyelid is associated with incompletely resections [18]. However, some authors have suggested Moh's micrographic surgery as an alternative to wide local excision. The tumors have a natural history of local invasion, and this risk remains high despite the use of Moh's surgery [19]. In a report by Bindra et al. [20], a patient presented with a PCMC that involved the lower eyelid in its entirety. The authors reported that wide surgical margins would be prohibitively morbid and instead opted for a 5-mm margin, which were free of malignant cells on histologic exam.
At our first operation, we excised the tumor with a simple 3-mm margin because the lesion appeared to be benign. However, histologic examination revealed the diagnosis of PCMC, and the patient underwent re-excision of the tumor site with an additional 3-mm margin from the initial scar. A wider surgical margin (i.e., 10 mm) was not acceptable to the patient who was worried about the resulting scar. We also thought that a wide excision could result in excessive facial scar, due to flap procedure, and also become a cause for ectropion. The patient was followed closely for 2 years, during which he experienced neither postoperative complications nor recurrence.
PCMC is a rare malignancy that can present as a benign skin lesion. Physicians should be aware of this tumor and be able to differentiate it from benign cystic or solid eyelid lesions.