INTRODUCTION
Craniofacial dermoid cysts are congenital or acquired developmental malformations containing the skin, and its appendages, such as the hair follicles, and sebaceous and sweat glands are commonly found in the lateral orbital region [1,2]. Dermoid cysts of the cranial bones are thought to develop from the entrapment of embryonic ectoderm along the cranial suture lines during fetal development, and those developing in the sphenoid bone are rare (3% of all dermoid cysts of craniofacial bone). In addition, they tend to be difficult to be found during early periods, since they are deep, slow-growing lesions [3,4].
They develop with a cutaneous sinus tract in rare cases [5], and dermoid cysts with a cutaneous sinus tract in sphenoid bone have been reported to date in only a few cases [3,4,6,7]. In such cases, an approach aimed to preserve the frontal branch of facial nerve, and to achieve a radical but aesthetic resection of the extracranial and intracranial lesion may be required, however, to the best of our knowledge, no report has been reported to date.
Herein, we present a rare case of a frontotemporal dermoid cyst in a child with a cutaneous sinus tract across the frontal branch of the facial nerve and deep extension through the sphenoid bone. The cyst was successfully resected with preservation of the nerve using two approaches (lateral orbital skin and temporal hair-bearing area). We achieved good results, and the approach was radically curative and aesthetically effective.
CASE REPORT
A 5-year-old boy had a congenital subcutaneous tumor in the frontotemporal region. Three years prior, it was swollen due to infection several times, and it was drained each time as an infectious atheroma at a local clinic. Thereafter, he was referred to our hospital due to repeated infection. At the initial visit, the tumor was associated with pus and infection, and its subcutaneous size was 1.5 cm├Ś1.5 cm. The patient had no significant past medical history, except for the tumor.
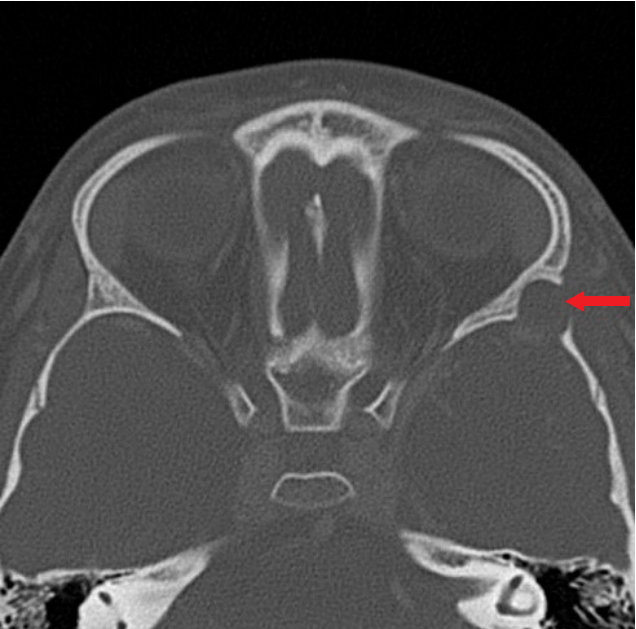
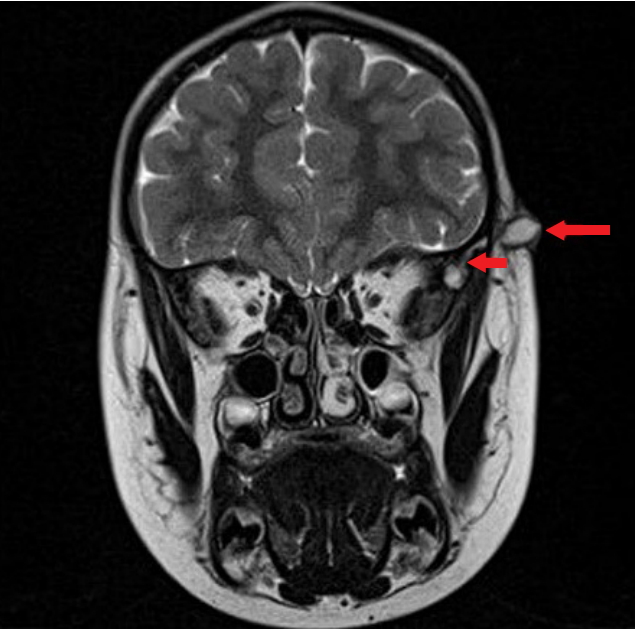
Computed tomography (CT) demonstrated subcutaneous cystic lesions as low-density areas and the lesion of sphenoid bone as a bony defect (Fig. 1). Magnetic resonance imaging (MRI) demonstrated a cystic lesion with a cutaneous sinus tract ranging from the subcutaneous tissue to temporal fossa, as a low signal in the T1-weighted image and as a high signal in the T2-weighted image (Fig. 2). The CT and MRI findings were suggestive of a dermoid cyst of the sphenoid bone with a cutaneous sinus tract. Furthermore, the images and location of the skin lesion suggested that this tract traversed medially across the course of the frontal branch of the facial nerve since this nerve locates between the line running from 5 cm above the upper border and lateral position of eyebrow to the tragus and the line running from the median height and lateral position of eyebrow to the earlobe base [8,9].
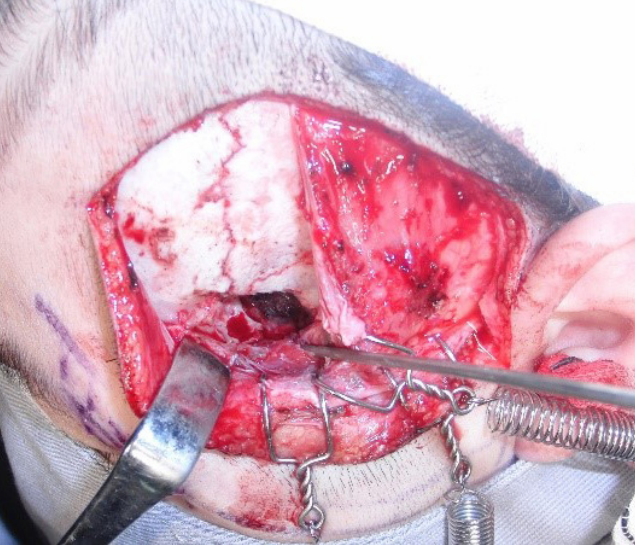
After controlling the infection, tumorectomy was performed, in cooperation with a neurosurgeon, under general anesthesia. We planned resection of the subcutaneous tumor above the cranial bone using a tumor marginal incision and the sphenoid bone lesion using an incision in the temporal hair-bearing area, which marked the course of the frontal branch of the facial nerve as described above (Fig. 3). The cutaneous sinus tract was carefully dissected thorough the skin, subcutaneous tissue, and temporal muscle with the preservation of the facial nerve (Fig. 4). Subsequently, the temporal hair-bearing area incision and underlying periosteum secured a surgical field enough to resect the lesion of the sphenoid bone. The sphenoid periosteum was incised, and subsequently, the sphenoid bone around its fistula was shaved off and the sphenoid cyst was exposed. The sphenoid cyst was in contact with the dura; however, it could be resected without rupture of the dura. Additionally, superficial electrocautery of the dura was performed to prevent recurrence (Fig. 5). Following saline irrigation and replacement of suction drain, skin closure was performed.
DISCUSSION
Dermoid cysts of the cranial bone rarely develop with a cutaneous sinus tract, and subcutaneous infection in 15% of such cases often make patients recognize its occurrence [5]. Their main lesion located in the deep layer cannot be found by visual examination and palpation, and it sometimes destroys the cranial bone and invades in to the dura [2,10,11]. Therefore, surgical removal in this region must be based on preoperative imaging.
CT can demonstrate dermoid cysts in low-density areas and the lesions of cranial bone are seen as bony defects [12]. MRI can demonstrate dermoid cysts as a low signal in a T1-weighted image and as a high signal in a T2-weighted image, and is suitable for detecting a cutaneous sinus tract [13]. Therefore, both CT and MRI are necessary for preoperative imaging in cases such as ours.
Complete resection of dermoid cysts of cranial bone with a cutaneous sinus tract often requires elaborate plans. A cutaneous sinus tract sometimes becomes complicated due to repeated infections, and the usefulness of methylene blue staining in diagnosis of a complicated tract has been reported [14,15]. However, in the present case, MRI demonstrated only one cutaneous sinus tract, and therefore, it could be exposed by using surgical bougie.
For the resection of large and deep cranial dermoid cysts, a wide surgical field should be secured in the point of radicality and safety. Large cranial defect needs augmentation with artificial bone, and definite invasion in the dura needs its resection and reconstruction. In the present case, cranial reconstruction was not needed since cranial defects were comparatively small and the temporal muscle was preserved. Furthermore, the tumor could be resected without rupture of the dura, and only superficial electrocautery to the dura was performed to prevent recurrence.
Frontotemporal dermoid cysts with a cutaneous sinus tract in sphenoid bone have been reported to date in only a few cases, however, the spreading of these lesions across the frontal branch of the facial nerve has not been reported. An appropriate approach is required to ensure preservation of this nerve, safety, radicality, and aesthetic outcome.
With these considerations, we completely resected the cutaneous tumor with a sinus using minimum skin incision and the cranial tumor with securing a wide surgical field by a hair-bearing area incision. Furthermore, long postoperative period with no recurrence and a good aesthetic outcome have been observed.