INTRODUCTION
The zygomatic arch is formed by the temporal process of the zygomatic bone and the zygomatic process of the temporal bone. It is located laterally in the face and is crucial in determining its width and prominence [1]. The zygomatic arch is a cylindrical, thin, and long bridge-like structure that is structurally vulnerable to local trauma; fractures commonly result from both high- and low-velocity forces [2]. Zygomatic arch fractures often occur as part of zygomaticomaxillary complex fractures, which account for approximately 25% of all facial bone fractures, whereas isolated zygomatic arch fractures comprise 10% of all zygoma fractures and 5% of all facial fractures [3–5]. Zygomatic arch fractures cause esthetic problems due to the facial asymmetry resulting from lateral facial flattening and depression in the affected area and functional problems due to coronoid impingement [1,3,4]. Despite the esthetic and functional importance of the zygomatic arch, a textbook classification of isolated zygomatic arch fractures has not yet been established. To date, five studies have presented zygomatic bone fracture classifications, and only two focused on isolated zygomatic arch fractures [6–10]. However, only one of those proposed classifications includes the injury vector, although this is one of the most important factors to consider in fracture cases. Furthermore, the only classification that does include the injury vector is too complicated to be suitable for daily practice. In addition, the existing classifications are clinically limited because they do not consider greenstick fractures, nondisplaced fractures with fracture lines only, or coronoid impingement. In the present study, we present a rearrangement of the previously published classifications and propose a modified classification of isolated zygomatic arch fractures that maximizes the advantages and overcomes the advantages of previous classification systems. We refer to this system as the Nam and Jung classification.
In the present study, we analyzed the major classification criteria (displacement, the force vector of the injury, V-shaped fracture, and coronoid impingement) of isolated zygomatic arch fracture subtypes from the five previous papers and created a modified classification system based on them. Using this modified classification, isolated zygomatic arch fractures of patients who visited our hospital were classified, and the usefulness of the new classification was confirmed by investigating the cause of injury, the operation rate, and surgical outcomes for each type.
METHODS
In this study, the classification criteria for isolated zygomatic arch fracture reported in five previous studies were analyzed, rearranged, and supplemented to develop a modified classification (Table 1, Fig. 1). For ease of comparison, we presented the modified classification system proposed herein (the Nam and Jung classification) together with the previous classifications in Table 1.
After obtaining approval from the Institutional Review Board of our institution (IRB No. 2021-10-021), this study analyzed patients with isolated zygomatic arch fractures who visited the blinded for review from January 2010 to December 2019. The epidemiology of isolated zygomatic arch fractures was investigated in 134 patients based on the medical records, the findings of radiographs and computed tomography (CT) of the facial bone (Table 2). Thereafter, the fractures were classified into subtypes according to the newly proposed classification (Figs. 2, 3) based on representative axial facial bone CT patient images. Finally, based on the classification presented herein, the associations of each fracture type in the modified classification with the cause of injury, the surgery rate, and surgical results were analyzed (Tables 3,–5). The causes of injury were subdivided into violence, fall/slip down, sports, traffic accidents, bicycle accidents, and other causes.
The surgical results were investigated according to the success of reduction as evaluated by a radiographic examination and symmetry as determined by a visual assessment immediately after surgery and at outpatient visits at 3 weeks postoperatively. The results were categorized as excellent (complete recovery of the alignment of the bone and arch shape on radiographs and symmetry in appearance), moderate (almost full recovery of the alignment of the bone and arch shape on radiographs and symmetry in appearance), or poor (incomplete recovery of the alignment of the bone and arch shape on radiographs and asymmetry in appearance due to under- or over-correction).
Statistical analyses were performed using SPSS version 28.0 (IBM Corp., Armonk, NY, USA) with the significance level set at p<0.05.
RESULTS
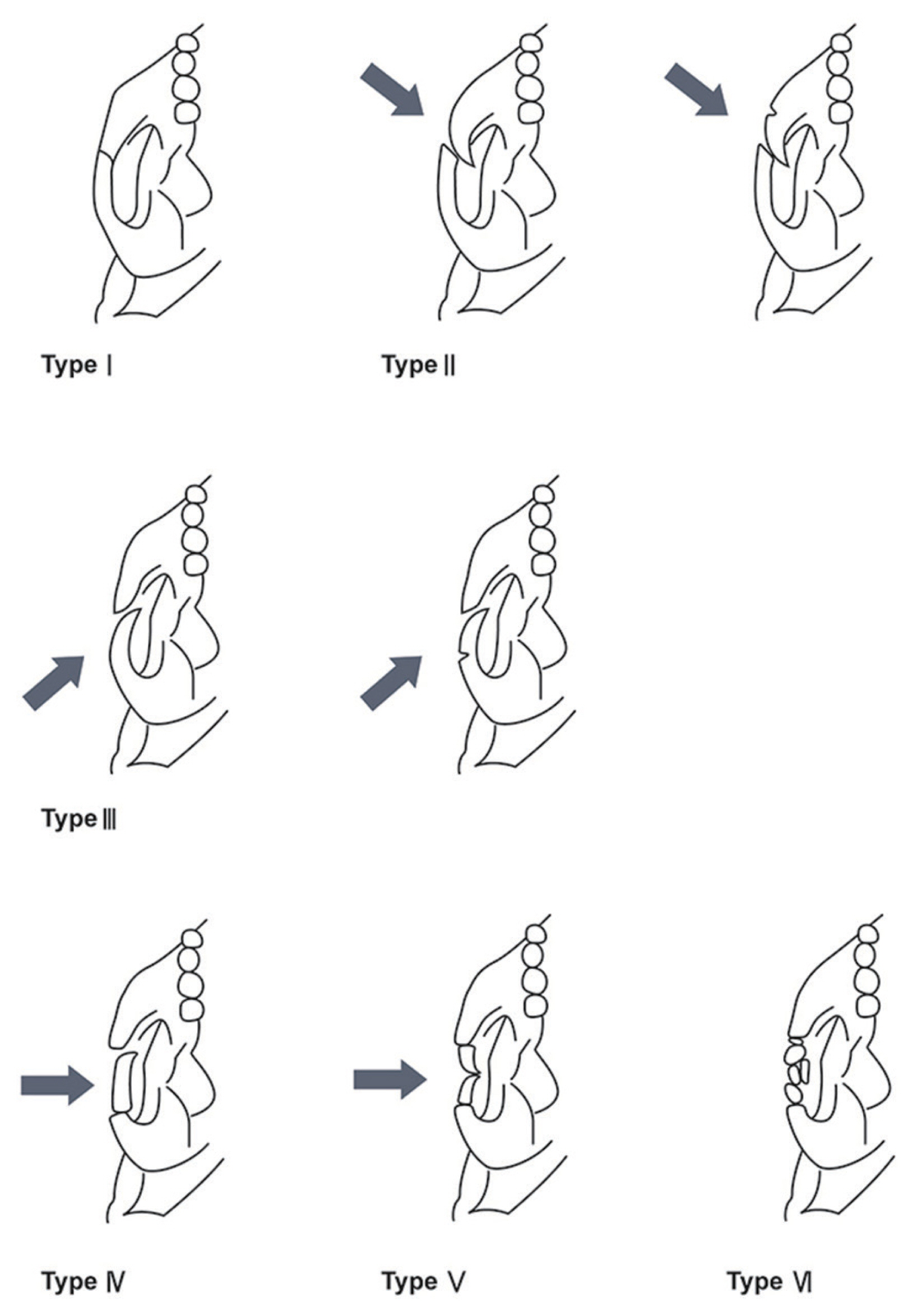
The major classification criteria for the isolated zygomatic arch fracture analyzed from the five previous studies included displacement, the force vector of the injury, V-shaped fracture, and coronoid impingement. A modified classification was developed by rearranging the previous systems and including all the major factors (Table 1). Based on these criteria, the newly proposed Nam and Jung classification subdivides isolated zygomatic arch fractures into six types (Fig. 1) as follows: (1) type I, nondisplaced fractures with fracture lines only or greenstick fractures with or without coronoid impingement; (2) type II, depression of the anterior portion and bone displacement with fracture lines or greenstick fractures due to injury with the force vector directed toward the anterior portion with or without coronoid impingement; (3) type III, depression of the posterior portion and bone displacement with fracture lines or greenstick fractures due to injury with the force vector directed toward the posterior portion with or without coronoid impingement; (4) type IV, depression of the middle portion and bone displacement with fracture lines or greenstick fractures due to injury with the force vector directed toward the middle portion with or without coronoid impingement; (5) type V, a V-shaped fracture with depression of the middle portion and bone displacement with fracture lines or greenstick fractures due to injury with the force vector directed toward the middle portion with or without coronoid impingement; or (6) type VI, comminuted fracture with or without coronoid impingement.
Epidemiological data on isolated zygomatic arch fracture are shown in Table 2. Of the 134 patients, 98 were male and 36 were female (age: 11–92 years; average age: 46.92 years). The fracture was on the right side in 66 cases (49.3%) and on the left side in 68 cases (50.7%). The causes of injury were violence in 17 cases (12.6%), fall/slip down in 63 cases (47.0%), sports injuries in 10 cases (7.5%), traffic accidents in 26 cases (19.4%), bicycle accidents in 10 cases (7.5%), and other causes in eight cases (6.0%). Conservative management was used for 53 cases (39.6%) and surgery for 65 cases (48.5%). Sixteen cases (11.9%) fell into neither category due to transfer to another hospital, refusal to undergo surgery, or loss to follow-up.
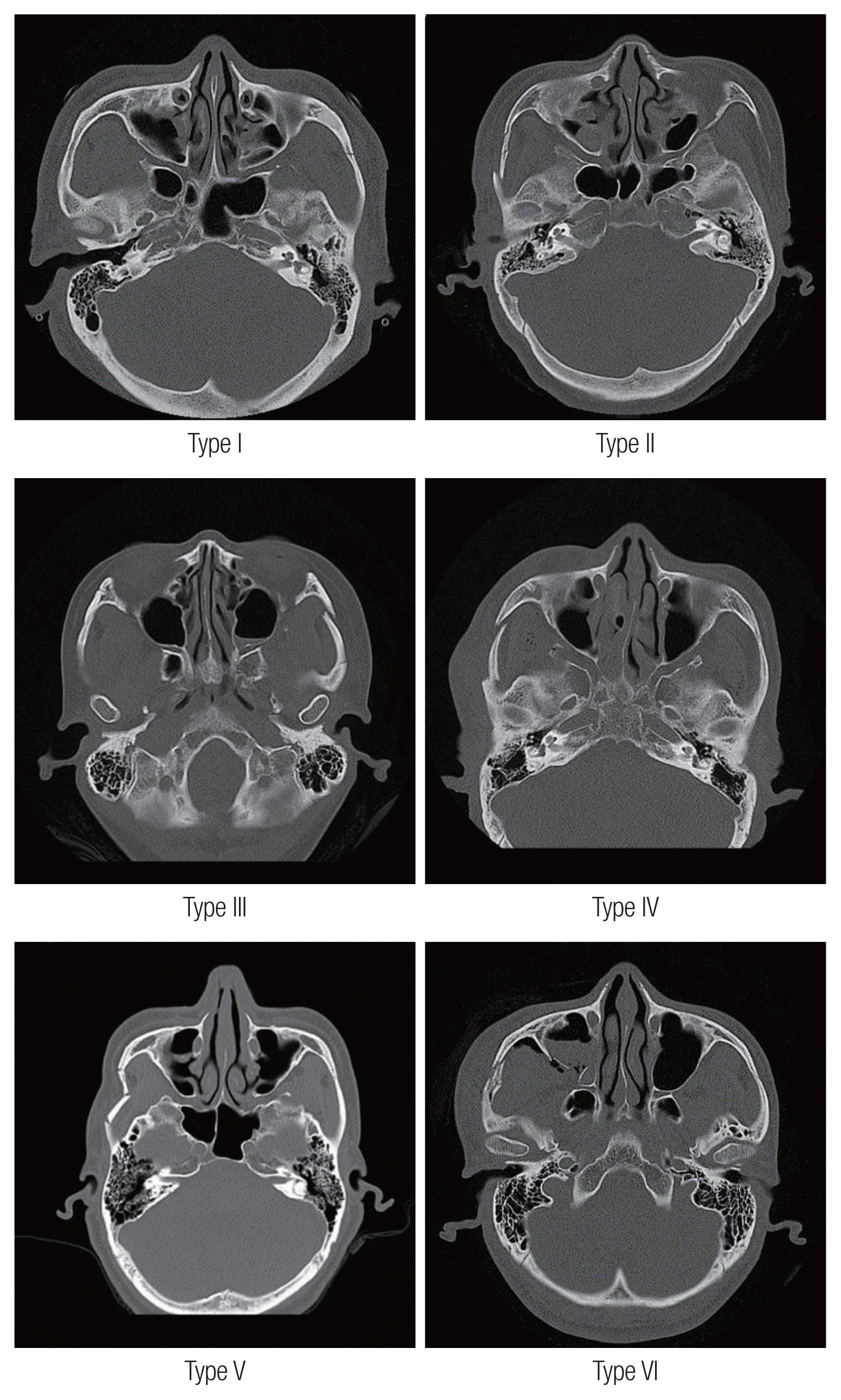
Axial facial bone CT images of representative cases of each type in the modified classification system are shown in Fig. 2. Table 1 presents a comparison between the previous systems and the newly proposed Nam and Jung classification, which includes all major classification criteria (displacement, force vector of injury, V-shaped fracture, and coronoid impingement) identified in the five previous papers.
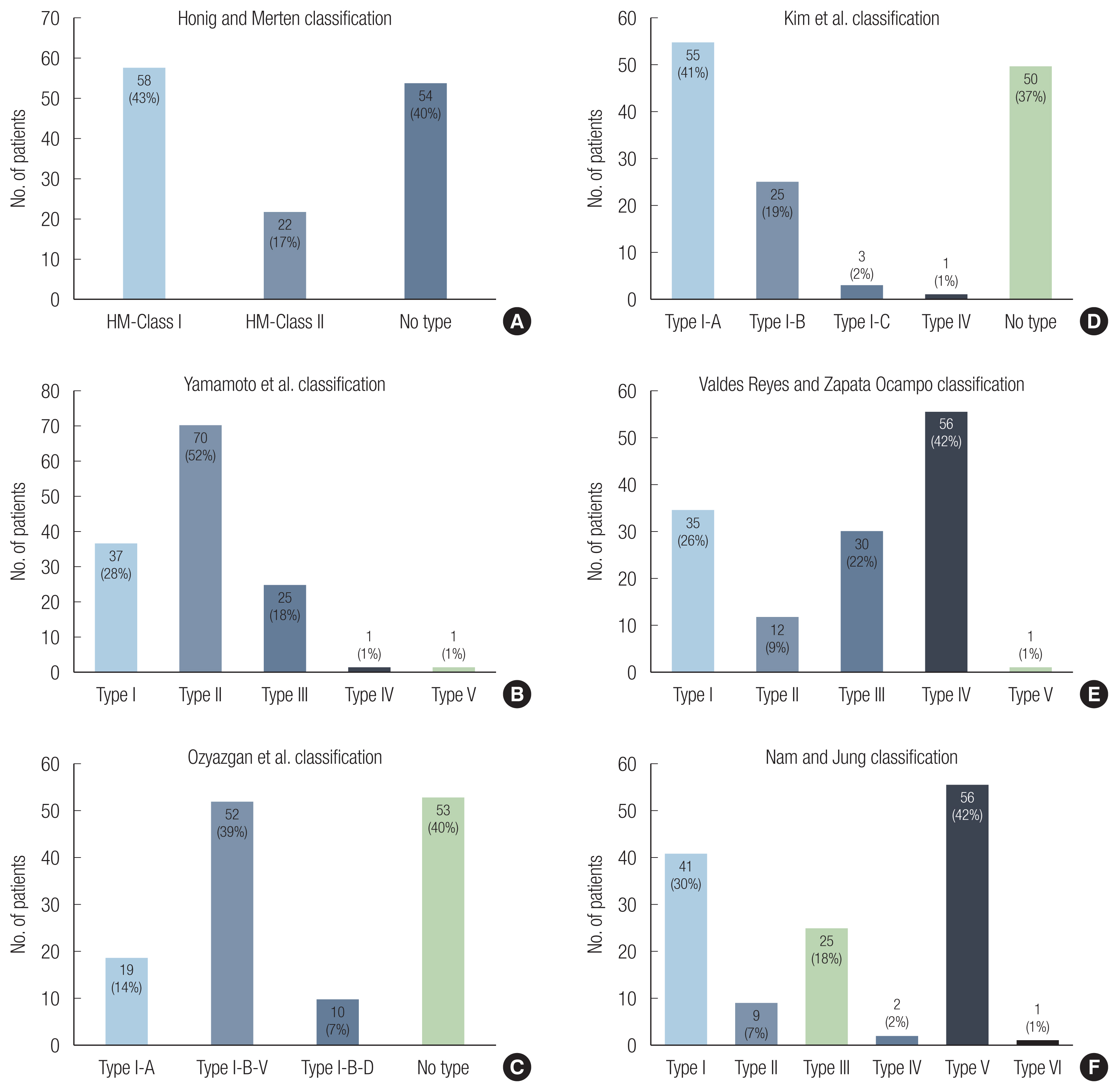
Fig. 3 shows the categorization of patients at our hospital based on the previous and modified classifications. The patients with isolated zygomatic arch fracture who visited our hospital were classified according to the modified classification (type I [n=41]; type II [n=9]; type III [n=25]; type IV [n=2]; type V [n=56]; and type VI [n=1]).
The causes of injury, the operation rate, and surgical results for each type of fracture in the modified classification are shown in Tables 3, 4, and 5, respectively. In types I, II, III, and IV, the most common cause of injury was fall/slip down, followed by traffic accidents. In type V, fall/slip down was also the main cause; however, the second most common cause was sports. Type VI was only identified in one patient, who had a fall/slip-down injury. The operation rate according to each type was as follows: type I, 4.9%; type II, 44.4%; type III, 52.0%; type IV, 100%; type V, 76.8%; and type VI, 100%. The causes of injury did not differ significantly among types (p=0.335) (Table 3), but the operation rate was significantly different (p<0.001) (Table 4).
Surgical treatment was performed in 65 out of 134 patients; the surgical outcomes according to each type are shown in Table 5. Surgical treatment was performed with closed reduction via the Gillies approach in 61 patients, and open reduction and internal fixation using a plate was performed in four patients (one with a type IV fracture, two with type V fractures, and one with a type VI fracture). The number of surgical outcomes classified as “moderate” increased significantly with greater severity (higher type, p=0.049). All data related to this study are available from the corresponding author upon reasonable request.
DISCUSSION
A classification system should facilitate clear communication; it should not be confusing and should be capable of including as many cases as possible. Most facial bone fracture patients first present to the emergency room, and a clear classification system that conveys a substantial amount of information about fractures would make it possible to classify patients more accurately in a primary care setting, thereby enabling smooth communication among medical staff. Furthermore, implementing a clear and well-organized classification system would facilitate analyses of existing patient data to obtain insights into the impact of each element constituting the classification system on fractures and their outcomes. Therefore, a clear and systematic classification can also improve data quality [11].
In this study, to maximize the advantages of the classification systems reported by previous studies and overcome their limitations, we propose a modified classification that divides isolated zygomatic arch fractures into six types based on bone displacement, the force vector of the injury, coronoid impingement, and fracture morphology.
The position of bone displacement is determined by magnitude and vector of the force causing an injury, and the key principle behind fracture reduction is to apply a force opposite the vector of trauma [12]. Therefore, bone displacement and the force vector of the injury are the most important factors to consider when classifying isolated zygomatic arch fractures. Two important masticatory muscles (the temporalis and masseter muscles) are related to the zygomatic arch [13]. When the zygomatic arch fractures, direct bone-to-bone contact with the coronoid process of the mandible may result depending on the fracture position, resulting in sudden coronoid impingement. In zygomatic arch fractures with coronoid impingement, if there is a severe limitation in mouth opening, even a minor fracture may require surgical treatment [1]. Hence, coronoid impingement is also an important consideration in zygomatic arch fractures. Finally, in our study, the commonest cases of fractures were separately classified into single types for ease of communication. To date, five papers have presented the classification of subtypes of zygomatic arch fractures, and only two among them attempted to classify isolated zygomatic arch bone fractures.
A study by Honig and Merten [6], which was published in 2004, classified zygomatic arch fractures into three classes based on radiological images, and only classes I and II included isolated zygomatic arch fractures. The Honig and Merten classification, which was the first classification to include subtypes of zygomatic arch fracture, was based on fracture morphology and displacement. The Knight and North classification [14], the Fujii and Yamashiro classification [15], and the classification of Zingg et al. [16] were also published; however, these systems only classified zygomatic arch fractures into a single type, without separate subdivisions. Furthermore, in the Honig and Merten classification [6], valid treatment plans and management strategies according to the types are presented, which is valuable for surgeons in treatment planning. However, the Honig and Merten classification is not solely for isolated zygomatic arch fractures and does not consider the vector of injury, which is crucial for reduction. The Honig and Merten classification also does not include cases with greenstick fractures or nondisplaced fractures under any subtype or consider coronoid impingement (Table 1).
In 2007, Yamamoto et al. [7] classified isolated zygomatic arch fractures into five types based on radiological images. This was the first classification of isolated zygomatic arch fractures, and their system considers bone displacement, contact, and the fracture line. However, the vector of injury and coronoid impingement are not considered. Greenstick fractures cannot be included under any of the subtypes, which remains a disadvantage of this classification (Table 1).
In a 2007 study by Ozyazgan et al. [8], based on radiological images, zygomatic arch fractures were classified into six types including subtypes. In this system, only type I-A, type I-B-V, and type I-B-D correspond to isolated zygomatic arch bone fractures. Ozyazgan et al. [8] presented a separate class for V-shaped fractures, which is the most common type of isolated zygomatic arch fractures. For convenience of communication among medical staff, the researchers proposed valid treatment plans and management strategies according to each type. However, their system does not solely classify isolated zygomatic arch fractures, and cases with greenstick fractures or nondisplaced fractures cannot be included under any type. Moreover, the vector of injury and coronoid impingement are not considered (Table 1).
Kim et al. [9], in 2014, based on radiological images, classified zygomatic arch fractures into eight types with distinct subtypes, of which only type I-A, type I-B, and type I-C include isolated zygomatic arch fractures. However, the classification of Kim et al. does consider the vector of injury. They also proposed valid treatment plans and management strategies according to each type to support surgeons. However, similar to previous classifications, this classification system also does not only consider isolated zygomatic arch fractures. Moreover, they also failed to address cases with greenstick fractures or nondisplaced fractures, as well as coronoid impingement (Table 1). Finally, despite the usefulness of subdividing fracture types according to the different force vectors of injury, the system of Kim et al. is too complicated to be suitable for daily practice.
In the present study, three major force vectors that induce isolated zygomatic arch fractures were considered. In 2020, Valdes Reyes and Zapata Ocampo [10] classified isolated zygomatic arch fractures into five types. This was the second and most recent classification of isolated zygomatic arch fractures alone. Moreover, it was the first classification to consider greenstick fractures and coronoid impingement. However, it has the limitation that it does not consider the vector of injury (Table 1).
Therefore, we maximized the advantages of each classification, analyzed and overcame their limitations, and proposed a modified classification (the Nam and Jung classification), as shown in Table 1. This modified classification system divides zygomatic arch fractures into six types based on bone displacement, the force vector of the injury, coronoid impingement, and fracture morphology. None of the previously proposed classifications include all the major criteria that influence isolated zygomatic arch fractures. Our rearranged classification system is accurate and intuitive, as it contains the major factors that should be considered and is capable of classifying as many cases as possible.
Using this classification, we analyzed the causes of injury, operation rate, and surgical results for each fracture type. The causes of injury did not differ according to type (Table 3), but the operation rate did show a significant difference (Table 4). Table 5 presents the surgical outcomes according to the new classification and shows that the frequency of outcomes classified as moderate increased significantly from fracture types I (a minimal fracture caused by a weak injury force) to VI (a comminuted fracture caused by a strong injury force). This suggests that bone displacement, dislocation, and coronoid impingement are more likely to occur due to middle force vectors than anterior and posterior force vectors, in that the surgical rate and the frequency of “moderate” surgical outcomes of types IV and V of the Nam and Jung classification, newly proposed in this paper, were significantly higher than those of types II and III. This further implies that in addition to the injury force, the injury force vector also significantly influences bone displacement, dislocation, and coronoid impingement. This renders a classification considering the injury vector meaningful.
In the management of isolated zygomatic arch fractures, the surgical decision depends on the operator’s subjective judgment, and the same treatment method can be used to successfully manage multiple fracture types. Furthermore, owing to the retrospective nature of this study, which included patients who completed treatment after developing a rearranged classification including all major criteria presented in previous papers, a limitation is that the treatment method cannot be generalized for each fracture type. To overcome this limitation, we analyzed the causes of injury, operation rate, and surgical results for each fracture type in the modified classification. We found that both the injury force and the injury force vector had meaningful effects on the operation rate and severity of injuries.
In conclusion, the new classification system presented in this paper includes the injury vector, which is the most important vector for reduction, and allows an intuitive consideration of reduction during the classification itself. In addition, this can be considered a functional classification system, since it considers both the injury force and vector. However, a limitation of the present study is that it did not present treatment plans and management for each type; further studies should develop an algorithm for this purpose.