INTRODUCTION
Nodular fasciitis is a self-limiting, non-neoplastic, reactive proliferation of connective tissue involving the subcutaneous or superficial fascia [1]. It can appear in any anatomic region but is most commonly found in the extremities or the trunk [1]. Nodular fasciitis is relatively uncommon in the head and neck lesions and many authors report a prevalence of about 7% to 15% [2,3,4,5,6]. Nodular fasciitis is often mistaken as a sarcomatous lesion due to its rapid growth, rich cellularity, high mitotic activity and poorly circumscribed nature [5]. These malignant-like characteristics may lead to inappropriate, aggressive treatment which may cause psychological and physical morbidity to a patient. Therefore, we should be aware of the clinical and pathologic character of nodular fasciitis and should make accurate diagnosis prior to treatment.
CASE REPORT
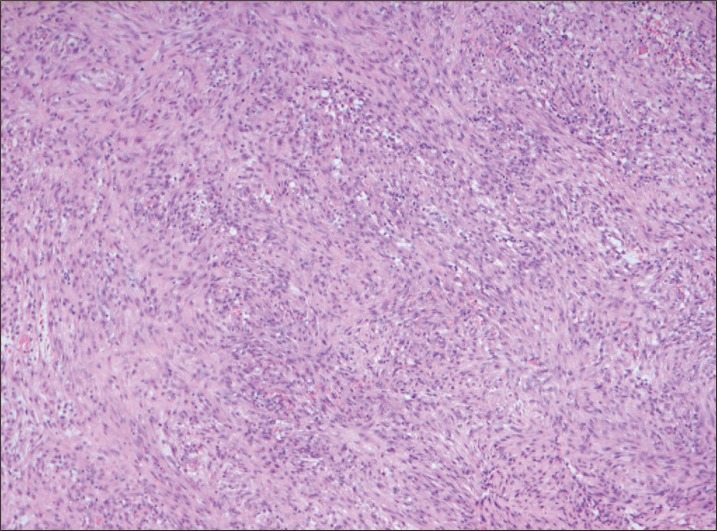
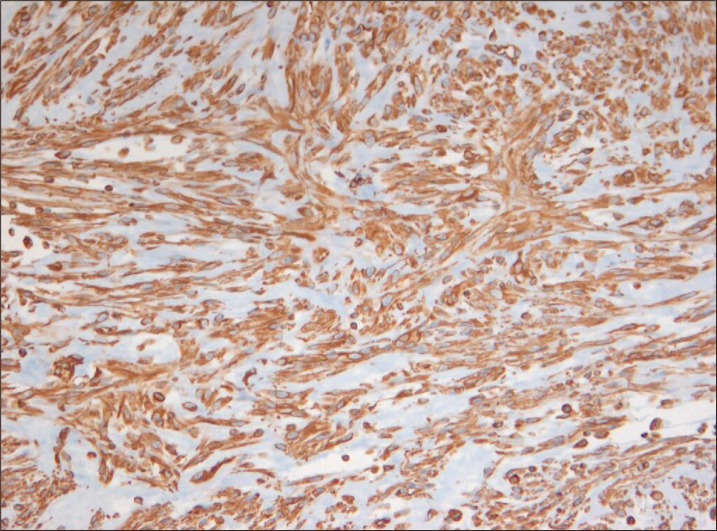
A 35-year-old man presented a mass at the medial side of the right upper eyelid (Fig. 1). It was found incidentally approximately three months prior. Since then the lesion grew rapidly and the patient was referred to our department to exclude the possibility of a softtissue malignancy. On physical examination, a mass of approximately 2.0 cm in size with firm and non-tender nature was noted. Paresthesia was noted over the forehead and scalp region of the supratrochlear nerve. Mechanical ptosis of the right upper eyelid was observed, but without any other abnormal findings on the general ocular examination. On computed tomography, a well demarcated 2.0 cm-sized, contrast-enhanced subcutaneous mass of the right supraorbital area was detected with no adjacent bony destruction (Fig. 2). Before the excision, punch biopsy was performed and nodular fasciitis was confirmed. A complete excision was performed under general anesthesia and the defect was closed primarily by local flap coverage. Macroscopically, the tumor was 1.5×1.8×1.5 cm in size and was well circumscribed, non-encapsulated with rubbery to myxoid texture (Fig. 3). The histological results showed the nodular proliferation of plump and spindled fibroblasts arranged in long fascicles with whorled appearance (Fig. 4). Frequent mitiotic figures were observed with scattered lymphocytes and extravasated red blood cells. Immunohistochemical study was performed, and the lesion stained positive for vimentin and smooth muscle actin but negative for cytokeratin, S-100 protein, desmin, and CD34 (Fig. 5). The patient underwent close observation and the resolution of the mass left only minimal scarring on the right periorbital area. The preoperative symptoms of mechanical ptosis and paresthesia over the forehead and scalp area subsided (Fig. 6). The postoperative follow-up was maintained up to 1 year after excision and no recurrence was detected.
DISCUSSION
Nodular fasciitis was first described by Konwaler et al. [2] in 1955, and it has been referred to as pseudosarcomatous fasciitis, peudosarcomatous fibromatosis, proliferative fasciitis or infiltrative fasciitis. This disease occurs primarily in adults in the third and fourth decades of life, regardless of sex [4]. It can develop in any area but there is a prevalence of observed cases in the upper extremities and the trunk [5,6,7]. Only approximately 7% of nodular fasciitis are found on the head and neck areas and such cases generally occur in young children [5,6,7,8,9]. Nodular fasciitis is especially uncommon in the periorbital area, only accounting for less than 1% of all periorbital masses [1]. The lesion ranges from 0.5 to 10.0 cm in size, with most being less than 4 cm with preclinical course of 4 weeks or less [10]. Although specific causes have not been reported, a history of trauma was found in approximately less than 1.5% of cases. In computed tomography or magnetic resonance imaging findings, the mass is well defined and homogeneous without invasion to adjacent tissues [11]. The histologic characteristics of nodular fasciitis include proliferation of spindle cell fibroblasts, frequently arranged in parallel bundles extending to all directions, and numerous mitoses of the spindle cell nuclei may also be seen [1]. The proliferation of capillary blood vessels and lymphocytic infiltration and extravasated red blood cells are also detected [4]. In immunohistochemical study, spindle-shaped fibroblasts in nodular fasciitis were shown to be positive for vimentin and sometimes actin but negative for keratin or S-100 protein [4].
Since the disease can be completely healed by a single surgical resection, the recommended treatment is complete conservative excision [5]. Following complete excision, local recurrence is reported to be rare [12]. Even in cases where complete resection could not be performed, it is usually resolved within a few months [13]. However, due to its rapid growth and the histopathologic similarity, nodular fasciitis could be misdiagnosed as a malignancy and an aggressive treatment may be inappropriately performed. Yoo et al. [4] have also previously reported that one must take caution of the possibility of such misdiagnosis, especially like in our case where a nodular fasciitis has occurred in an aesthetically prominent region such as the periortbital area. It is important that a treatment plan is established through an accurate diagnosis to avoid an unnecessarily aggressive treatment and to lead to an aesthetically favorable result. Also, according to Gelfand et al. [6] spontaneous regression can occur in some cases after incomplete excision; therefore it is possible to hold a surgical procedure and wait for regression under close observation. Other authors suggested steroid as a treatment option as well [14]. They published a case of nodular fasciitis on the arm that responded to intralesional steroid with complete resolution in 36 hours. Such method may act as an alternative treatment for nodular fasciitis in cases where a complete excision is difficult, and this treatment may also be applied to aesthetically important areas such as the head and neck.
In this article, we report a case of relatively uncommon periorbital nodular fasciitis that occurred in an adult. Although cases of fasciitis in the orbital area occur with lower than 1% probability, it is still important to suspect nodular fasciitis and to establish a proper treatment plan after an accurate diagnosis. Such careful steps will reduce unnecessary psychological morbidity and lead to aesthetically favorable results.