INTRODUCTION
Unilateral nostril hypoplasia is an extremely rare congenital malformation that may affect the soft tissue, cartilaginous, and/or bony structures of the nose. Manifestations can vary widely, with severe cases involving total obliteration of soft tissue and malformation or cleft of underlying structures including premaxilla and choanae. This deformity is very rare, but can occasionally be found in atypical cases with cerebro-oculo-nasal syndrome, interhemispheric fusion, or craniofacial cleft [1,2]. Because of this, surgical techniques for correction of this deformity have been limited to few case reports, which include Z-plasty, local flaps, cheek rotation flap, rotation and advancement flap, and tissue expansion [3,4,5,6]. We report a case of unilateral nostril hypoplasia in a patient whose nasal obstructive symptom was dramatically improved by Z-plasty.
CASE REPORT
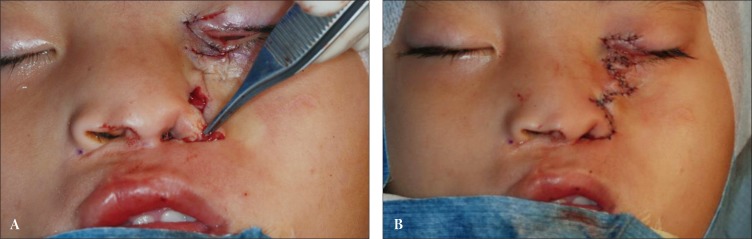
A 7-year-old Vietnamese girl presented with left-sided nostril hypoplasia at Lao Cai Hospital in Vietnam while senior author was providing volunteer medical services (Fig. 1). The guardians were unable to give any history relevant to family history or hereditary syndromes. The child had inferiorly displaced medial canthus and lower eyelid coloboma, which made her left side of the midface appear shorter than the right side, as well as a superiorly displaced alar base and deformed alar rim (Fig. 1). She suffered from soreness and dryness in the left eye from the periocular deformities. The alar rim deformity was sufficiently severe to make breathing through the left nostril virtually impossible, and to cause the patient to appear as if she had a single nostril. During a second examination on the day of preoperative planning, a pinpoint opening was identified in the soft-tissue, and the patency was found to extend through the bony structure underlying the affected alar rim, which became a key functional indication for a construction of a new nostril.
The nasal and eyelid deformities were addressed by a sequence of Z-plasties. For repositioning the eyelid, Z-plasty was designed for the medial canthal area, and a discrete irregular Z-plasty was separately designed for the alar area (Fig. 2). Flaps and underlying facial expression muscles were carefully dissected. The superiorly-based nasofrontal flap was advanced and turned over to reconstruct the nasal ala, and a laterally-based cheek flap was advanced supero-medially to lengthen the perinasal midfacial area. At the same time, Z-flaps designed on medial canthal area were transposed to reposition the left medial canthus and to conceal the lower eyelid coloboma. Intraoperatively, nasal turbinates were slightly hypoplastic and choanal space was relatively well maintained on the affected side. Thus, sufficient space was obtained in the left nostril after transposing the Z-flaps on the left nasal ala. After confirming adequate passage of Nelaton catheter through the newly formed left nostril, transalar suture using absorbable stitch was performed on left ala to maintain the dimension of the opening. Immediately after the operation, wet gauze was packed to maintain the contour of newly-constructed left nostril (Fig. 3). The skin flaps survived without any complications, and the packing was removed on postoperative day 3. The patient was very pleased to find that breathing through the nose required much less effort. The senior author completed his volunteer services in Vietnam and returned to Korea several days after this. Subsequently, another medical team visited Vietnam for volunteer services and was able to follow-up with the patient (Fig. 4). The patient had recovered well after surgery and was satisfied with the results. The reconstructed eyelid and nostril were favorably maintained.
DISCUSSION
Nostril hypoplasia is an extremely rare congenital anomaly and may be associated with severe congenital syndromes. In this case, the underlying structures were scarcely affected, while soft tissue opening was nearly absent. Similar phenotypic appearances are also found in patients with craniofacial cleft [1,2]. There are several reports of patients with cerebro-oculo-nasal syndrome with abnormal nares, and Richieri-Costa and Ribeiro [7,8] had reported a case of atypical interhemispheric fusion with a functional single nostril [9]. However, the general facial appearances in those cases were different from the facial appearance of the patient presented here. On the other hand, craniofacial cleft patients have facial appearances similar to the preoperative facial appearance of this case.
The most widely accepted and easily applicable classification for facial cleft was proposed by Tessier [10] in 1976. The Tessier number 3 cleft is one of the most challenging malformations to reconstruct and is characterized by inferior displacement of the medial canthus, superior displacement of the alar base, cleft lip and palate, coloboma of lower eyelids, nasolacrimal abnormality, cleft of the inferomedial orbital wall, and teloorbitism [11]. The Tessier number 4 cleft has been reported in less than 50 cases in the literature and is characterized by laterally and inferiorly displaced canthus, upward rotated nasal ala, and cleft lip lateral to the Cupid's bow [12]. Based on previous reports, the present case appears to represent either a number 3 or 4 cleft on the clinical spectrum of Tessier clefts. To the best of our knowledge, this is the first report on the application of multiple Z-plasties in successful correction of facial cleft patient in Korea. Because of the rarity, surgical techniques regarding single nostrils are based on case reports, which include local flaps, cheek rotation flap, and tissue expansion. Z-plasty may be a simple but powerful tool to repair the key elements in most cases of nostril hypoplasia or Tessier number 3 cleft [1,13,14]. It can be used to correct ectropion, which may be a secondary consequence of a vertical loss of both the anterior and posterior lamellae of lower eyelids [13]. Also, Z-plasties can be chosen to repair the three main components of Tessier cleft 3 - the lower eyelid ectropion, the cleft lip, and the cleft between nose and malar area [1,14]. In our case, we designed two asymmetric Z-flaps, one containing the nasal alar segment and another on the nostril base. By transposing each flap, the abnormal nasal ala was rearranged to restore symmetry in the midface, while successfully constructing a nostril. The discrete Z-plasty on left medial canthal area contributed to elongation of the left midface.
In conclusion, the fundamental principle in correcting single nostril is a precise diagnosis, including genetic analysis and the identification of accompanying anomalies, followed by thorough examination of the nasal components before detailed surgical planning. Because of the wide variation in anatomic configurations, the correction of single nostril should be individualized to achieve optimal results. The present case shows that Z-plasty may be a simple and powerful tool in cases of single nostril.