Unusual Bilateral Impalement Injury with Rusted Iron Bars on Face and Neck
Article information
Abstract
Impalement injury is the subset of penetrating trauma, defined as fixed, elongated objects penetrate and remain in the human body cavity or region by relatively low velocity. We report an unusual case of facial and neck impalement where two dirty rusted iron bars penetrated forehead bilaterally and exited neck and ear respectively without causing major organ injuries. After thorough radiologic and physical evaluation, the patient got medical and surgical treatment. The patient was discharged without complication after four day of delayed wound closure. There have been no complications and sequelaes related with trauma, wound infection and scar contracture at 3-year follow-up. According to affected organs and pattern of impalement, individualized and multidisciplinary surgical approach should be considered. Following these guidelines as in this case, it was possible to achieve excellent clinical outcome in impalement injury.
INTRODUCTION
Impalement injury is the subset of penetrating trauma, defined as fixed, elongated objects penetrate and remain in the human body cavity or region by relatively low velocity. Although impalement injury in face and neck is uncommon among civilian population in modern days, it could be associated with crush injury, wound contamination, and injury to major organs.
In this study, we will describe an unusual case of impalement injury, affecting face and neck bilaterally with dirty rusted iron bars, initially suspected to have caused major trauma. We also review the management and the treatment of the patient divided into pre-hospital and in-hospital stage.
CASE REPORT
A 69-year-old male with impalement injury with rusted iron rods on his face came to the emergency department. He was found by a passerby in upside down position with iron fence stuck in his forehead and body lean on the wall. The rescue team cut off the fence and took him to hospital. When he arrived at our hospital, the rusted iron bars penetrated through his forehead bilaterally. On the right side, the bar penetrated on the forehead in a downward angle running along the cheek and exiting through right ear, and on the left side, the bar out through the left mandible angle (Figs. 1, 2). Intravenous broad spectrum antibiotics were started and tetanus vaccination with tetanus immunoglobulin was injected. He was fully drunken but conscious and had no sign and symptom of brain and facial nerve injury. Facial bone and neck computed tomography (CT) scan revealed that there was no penetration of facial bone or skull, no injury of major vascular, and organ injury of face such as parotid glands. There were two dense radio-opaque metallic foreign bodies in both frontotemporal scalp with penetrating into right auricle and left masticator space and left lateral neck with no definite parotid gland penetration (Figs. 3, 4). He was admitted to the plastic surgical department and got emergent operation for removal of foreign bodies under general anesthesia (Fig. 5). After removal of the materials, the tunneling wounds on his both parietal areas were massively irrigated with normal saline and surgical drains were placed to prevent hematoma collection. The patient was treated with broad spectrum antibiotics and wound irrigation and debridement was done daily in operating room. At eleventh day after his trauma, he underwent a delayed wound closure under local anesthesia. Postoperatively the patient recovered well. Postoperative CT scan showed no sign of development of intracranial hemorrhage, hematoma, and the residual foreign bodies. His facial motor and sensory examination revealed normal findings. The patient was discharged without complication after fourth day of delayed wound closure. There have been no complication and sequelae related with trauma, wound infection and scar contracture at 3-year follow-up.

A 69-year-old male with penetrating injury with rusted iron rods on his head came to the Emergency Department

Preoperative plain radiologic image.

Facial bone computed tomography scan disclosed a radio-opaque foreign body penetrating through left frontoparietal area.

Facial bone computed tomography scan disclosed a radioopaque foreign body penetrating through left frontoparietal area. There was no penetration of the foreign body into left parotid gland (the blue arrows indicate both parotid glands).
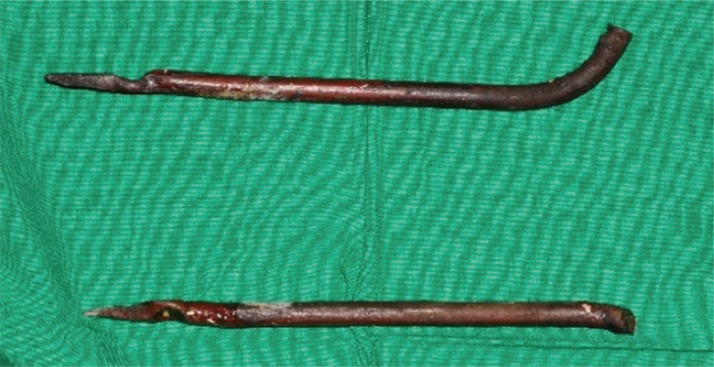
Removal of rusted iron bars: 18-cm from right (upper), and 23-cm from left (lower).
DISCUSSION
Eachempati et al. have divided impalement injuries into two types [1]. Type I injuries belong to the cases were the human body hits an immobile object, sometimes suspending the body off the ground. These type of injuries frequently results from unintentional falling or slipping onto protruding objects. Type II injuries occur when a stationary body gets penetrated by a moving object, e.g., traffic accidents. Our patient belonged to type I with his body suspended in the air.
Although the prognosis is usually favorable in the cases of the absence of damage in vital organs, initial assessment of impalement injury patients should be considered as major trauma patient before thorough neurologic, vascular, and airway assessment are completed. Therefore the most important pre-hospital management of patients are 'doing' and 'not doing' procedures to avoid further injuries. In our case, the patient was suspended by iron fence in upside down position for 5-6 hours. If a patient is found suspended on a penetrating object, measures should be taken on site, to try to reduce the strains on the body due to gravity. The object is fixed or immobilized, like our case; the size of the piercing object should be reduced. After that, 'not doing' any attempt to remove the object in situ before hospital. Because doing so could cause further damage surrounding vital tissues, particularly large blood vessels and nerves.
After the patient arrived at the hospital, thorough airway, breathing and circulation, neurologic, and vascular assessment was performed as major trauma patient. In impalements of head and neck, the airway should check meticulously even if initially thought to be intact.
Trauma wounds are usually contaminated or dirty. Some unusual yet possible consequences of maxillofacial infections are acute osteomyelitis, infected cavernous sinus thrombosis, and necrotizing cervical fasciitis [2]. As a higher prevalence of infections is observed in maxillofacial trauma wounds, starting intravenous "prophylactic" antibiotics is one of the first-line therapies after the patient arrive at the hospital. The choice of antibiotics was based on the potential type of infection. Because staphylococcal infection is the most frequent in facial soft tissue wounds, we used cephalosporin. Penicillin can be used only if there is concern for intraoral bacterial contamination [3]. Because tetanus is also a potentially lethal medical condition caused by penetrating injuries contaminated by dirt, feces, saliva, soil [4], tetanus toxoid and the tetanus immunoglobin were also given to the patient.
After initial assessment and medical treatment, the patient was proven stable; we considered operation for foreign body removal. To decrease the likelihood of infectious complications, surgical treatment should be performed within 12 hours of the accident, however large-sized impacted foreign body should not be removed without first performing a thorough radiologic investigation. Before the surgical procedure, we got information about the extent of damage and vital structures around foreign body with radiologic evaluation including X-ray skull, and CT scan. CT is typically the first-line radiologic examination for head-injured patients for surgical decision making such as the type of surgery, the route for extraction of the foreign body [56]. Our patient, especially on his left side, as the object entered on the forehead and penetrated in a downward along the cheek, was highly suspected of having injured the parotid gland before CT scanning. Postoperative use of CT scans proved useful in detecting residual foreign bodies as well as evaluating intracranial hematoma development. After surgical removal of dirty or rusted foreign bodies, our patient received daily debridement and wound irrigations. Infection is the most common late complication due to retained foreign bodies [7]. Foreign bodies can change the regional anatomy because they cause inflammatory response and subsequent scarring in surrounding tissue. These processes can leave some sequel such as deformity and functional impairment [8]. Therefore, foreign bodies in the maxillofacial area should be meticulously removed. After our patient's wounds demonstrated no evidence of infection and residual foreign bodies, we performed delayed wound closure. This method was successful because the patient has shown having no functional abnormality from injury of nerves and vessels; delayed wound infection related with residual foreign bodies; or facial deformity related with internal scar contracture.
In this article, we report an unusual case of facial and neck impalement where two dirty rusted iron bars penetrated forehead bilaterally and exited neck and ear respectively without causing major organ injuries. During all stages of treatment, care should be taken to perform immediate and systematic trauma evaluation, subsequent interventions should follow standard emergency trauma protocols. The primary rescuer 'do not' try to remove the piercing object and the patient should be brought to the hospital rapidly. At the hospital, initial assessments and medical treatment should be started as soon as possible and surgical treatments are considered based on the patient's condition. According to affected organs and pattern of impalement, individualized and multidisciplinary surgical approach should be considered. Following these guidelines as in this case, it was possible to achieve excellent clinical outcome in impalement injury.
Notes
No potential conflict of interest relevant to this article was reported.