INTRODUCTION
Microcystic adnexal carcinoma (MAC) was first described as a slowly growing but locally aggressive adnexal neoplasm in 1982 [1]. MAC is an uncommon type of tumor, with about 300 cases reported globally. MAC occurs in functionally and cosmetically sensitive anatomic locations, mostly on the face, so distinguishing between benign and malignant lesions for accurate diagnosis is important for proper patient management planning [2,3,4,5,6]. However, MAC is occasionally misdiagnosed as other benign or malignant neoplasms, such as desmoplastic trichoepithelioma, basal cell carcinoma, squamous cell carcinoma, and syringoma due to their histological similarity [3,4,7]. Here, we present a case of MAC misdiagnosed as desmoplastic trichoepithelioma on preoperative biopsy.
CASE REPORT
A 66-year-old woman with a mass on her face was transferred to us from dermatology for excision. There were multiple skin-colored indurate nodules in the right perioral area (Fig. 1). She had first noticed it 20 years previously. At that time, it was a small pimple-like mass. It had grown very slowly for 20 years since then. On palpation, the mass was firm, immovable, and located at the subcutaneous level.
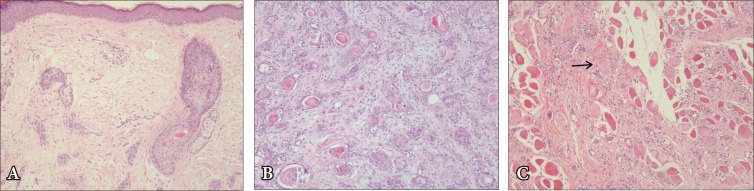
The lesion was diagnosed as desmoplastic trichoepithelioma in a preoperative punch biopsy carried out by a dermatologist (Fig. 2A). While immunohistochemistry can help distinguish MAC from other tumors, it was not done by our pathology department.
We performed an excisional biopsy of the lesion under local anesthesia. Contrary to our expectation, intraoperative findings showed that the lesion was ill-defined and invading the perioral muscles and vessels. We could not perform a complete excision due to the tumor's ill-defined margins and benign preoperative biopsy diagnosis. However, the postoperative biopsy showed that tumor cells had invaded the muscle layer and also showed perineural invasion, so the result was MAC (Fig. 2B, C).
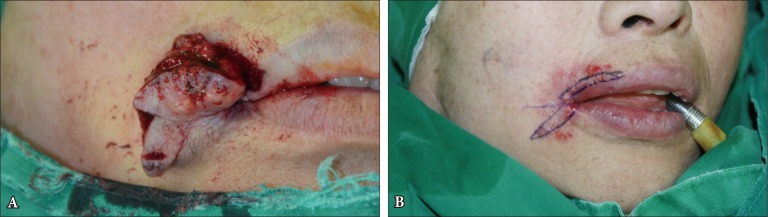
Based on these findings, we planned to make a wide excision under general anesthesia 12 days after the first operation. The incision was made along the vermilion border with margins of 2 mm from the previous incision line (Fig. 3). We resected not only the tumor but also the adjacent muscle, vessels, overlying lip, perioral skin and oral mucosa (Fig. 4). Resected tissues were sent for frozen biopsy, and there was remnant MAC tissue on the lateral margin. Therefore, we carried out another further resection of 2 mm from the lateral margin. The excised muscles were repaired, and defect of the lip was reconstructed by mucosal advancement flap.
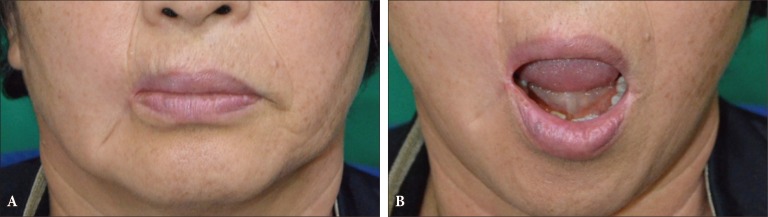
During the first 18 months after surgery, there was no significant complication or local recurrence. Although motion of the mouth was slightly restricted, the patient was satisfied with the results (Fig. 5).
DISCUSSION
MAC is an uncommon type of tumor. Generally, MAC can present variable features from a smooth flesh-colored or yellow plaque to a cystic nodule, as seen in this case. It was difficult to suspect MAC with only the clinical presentation of our patient, even with the result of desmoplastic trichoepithelioma on preoperative biopsy. However, because the feature of our patient-multiple nodules that grew for 20 years-is not commonly presented, the possibility of malignancy should be considered.
MAC rarely leads to death [8]. However, because it is malignant, complete resection with clear surgical margins must be done to prevent recurrence. Although, there is currently no clearly suggested resection margin for treatment. Multiple case series and one prospective study proved that treatment with Mohs micrographic surgery (MMS) results in a low recurrence rate [9]. Abbate et al. [10] reported that an MMS group showed a lower recurrence rate than a wide excision group. These results suggest that MMS is a reasonable first-line therapeutic modality for MAC [2].
There is no consensus regarding the follow-up period for MAC, but the recurrence rates for conventional excision may be as high as 47%, usually within the first 3 years. For MMS, the recurrence rates ranges from 0% to 22% with a 5-year follow-up [4,9]. The indolent course of the tumor is well described, and recurrences have been described 30 years after initial treatment. Therefore, irrespective of treatment modality, all patients should be monitored closely for several decades [10,11].
MACs are mostly located in the perioral and paranasal areas, which are functionally and cosmetically sensitive locations. Defects and deformities on the face resulting from wide excision are inevitable, despite the reconstructive efforts of surgeons. Clearly, accurate diagnosis and appropriate treatment are very important.
Superficial punch biopsy is a time and cost-effective procedure. However, it has led to a decrease in the size of tissue samples submitted for histopathologic examination. Also, it occasionally leads to difficulty in differential diagnosis because the pathologist cannot see the exact breadth or depth of the tumor. In one case study, misdiagnosis occurred in 27% of MAC cases, and that is secondary to inadequate sampling [2]. This is a limitation of superficial punch biopsy, and occasional misdiagnosis is inevitable. MAC shows pathologic findings that are similar to those of desmoplastic trichoepithelioma, and the depth is a critical clue for diagnosis.
Surgeons should be aware of the possibility of misdiagnosis and get informed consent from patients as the diagnostic change from benign to malignant is upsetting for them. In cases like MAC, surgeons should sufficiently inform and explain to patients for them to understand that their diagnosis may change depending on biopsy results.