Chondroid Syringoma on Face
Article information
Abstract
Chondroid syringoma is a rare mixed tumor of the skin which is composed of both mesenchymal and epithelial cells. Its incidence at less than 0.1% and is frequently located on the head and neck. Chondroid syringoma is easily confused with epidermal cysts. Since malignant forms of chondroid syringoma have been reported, accurate and timely diagnosis is important for proper management. We report clinical and histological features of chondroid syringoma in 5 patients treated at our institution. In most of the cases, chondroid syringoma presented as a round, firm, nodular or cystic lesion that had well marginated heterogeneity in sonography. Clinically, all of the lesions were removed by simple excision. Microscopically, all five tumors were well circumscribed and consisted of epithelial, myoepithelial, and stromal components. The epithelial component formed tubules lined by one or more rows of eosinophilic epithelial cells. The outer layer of tubules appeared to be flattened myoepithelial cells. The stroma is myxoid and contained spindle shaped myoepithelial cells. We expect that the clinical, sonographic, and histological data from our report may help clinicians who are confronted with various kinds of analogous facial lesions to decide the most proper management for their patients.
INTRODUCTION
Chondroid syringoma is a rare mixed tumor of the skin. It is composed of both stromal and epithelial cells. The incidence is quite low at 0.01 to 0.098 percent [1]. Chondroid syringoma presents as a slow growing, asymptomatic, round, firm, elevated, and movable mass. Because of these characteristics, chondroid syringoma can easily confused with epidermal cysts. However, Sungur et al. have reported that rapid growth, ulceration, and necrosis was evident at chondroid syringoma [2].
The lesions are most often seen in the head and neck region and have a predilection for male adults. Though these mixed tumors are usually benign, malignant forms have also been reported, most commonly when present in the extremities and the torso of younger patients with the female-to-male ratio being 2:1 for the malignant form. Barnett et al. have reported that malignancy is associated with 48% of regional lymph node metastases and 45% of distant metastases, most commonly to the lung and bone [34]. Therefore, accurate and timely diagnosis is important. Here, we report five cases of chondroid syringoma of the face treated by surgical excision.
CASE REPORT
In the past 7 years, our department has managed 5 cases of chondroid syringoma, which were reevaluated clinically and histologically for this report. We reviewed the medical records for demographic information, location and size of tumor, sonographic findings, and histopathologic results (Table 1).

Clinical characteristics
In Case 1, a 44-year-old man was referred for treatment of a palpable lesion that had been recurrent on the upper lip for a year. There was a history of trauma to the upper lip by an electric shaver a year prior to presentation. Physical examination showed a non-tender, round, elevated, and palpable nodule, measuring 1.2cm in diameter. The mass was excised and closed primarily. Histopathologic report was a chondroid syringoma.
In Case 2, a 39-year-old man presented with an elevated lesion on the nasal dorsum that had been growing slowly for 3 years. There was no history of trauma to the nose. On examination, the lesion was soft, fixed, and round which was 0.7 cm in diameter. Face sonography revealed an oval hypoechoic nodule in the deep dermal layer. The mass was extirpated and closed primarily. Histopathologic report was a chondroid syringoma.
In Case 3, a 47-year-old man was referred for treatment of a recurrent palpable lesion that had been on the upper lip for 2 years. There was no history of trauma to the upper lip. However, the patient had undergone incision and drainage of the lesion at a dermatology clinic. Physical examination showed a firm, round, movable, and protruded mass which was 1 cm in diameter and with postoperative scar on the left upper lip beside a philtral ridge. Face sonography revealed a well demarcated lesion without increased vascularity in the orbicularis superficialis muscle to the skin layer. The mass was excised and closed primarily. Histopathologic sectioning revealed a chondroid syringoma.
In Case 4, a 64-year-old man developed an elevated lesion on the philtrum for 6 months. There was no history of trauma to the philtrum. On examination, the lesion was non-tender, firm, and oval shaped, measuring 0.8 cm in diameter. The mass was excised and closed primarily. Histopathologic report was a chondroid syringoma.
In Case 5, a 65-year-old woman presented with an elevated lesion on the left nasolabial fold, which had grown slowly over 20 years. There was no history of trauma to the left nasolabial fold. Physical examination revealed a hard, movable, and round nodule, which was 2.2 cm in diameter (Fig. 1). Face sonography showed a well marginated heterogeneous solid nodule with multiple internal calcification in the left nasolabial junction (Fig. 2). The mass was extirpated and closed primarily. Histopathologic report was a chondroid syringoma (Figs. 3, 4).

Surgical specimen from Case 5. The mass was firm and measured 2.2 cm in diameter.

Face sonography in Case 5. The ultrasound exam revealed a well marginated heterogeneous mass with multiple internal calcification in the left paramedian nasolabial soft tissue.

Microscopic examination in Case 5. This chondroid syringoma has keratinous cysts and patchy calcifications (H&E,×.20).
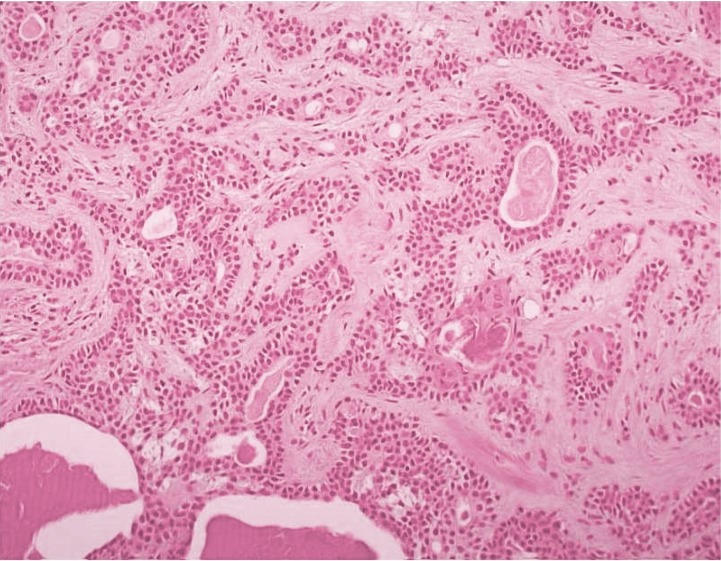
The chondroid syringoma is composed of ducts lined by epithelial and myoepithelial cells and myxoid stroma containing spindle myoepithelial cells with a small keratinous cyst (H&E,×.200).
DISCUSSION
In our review, most patients with chondroid syringoma presented with a round, firm, nodular or cystic lesion with well marginated heterogeneity on sonography. All instance of chondroid syringoma was surgically excised. Microscopically, all five tumors were well circumscribed and consisted of epithelial, myoepithelial, and stromal components. The epithelial component formed tubules lined by one or more rows of eosinophilic epithelial cells. The outer layer of tubules appeared to be flattened myoepithelial cells. The stroma was myxoid. It contained spindle shaped myoepithelial cells. Three out of five cases had keratinous cysts and foci of squamous differentiation. In one case, patchy calcification was observed.
Complete excision with a cuff of normal tissue remains the standard treatment for chondroid syringoma [5]. However, all five cases in our report were removed by simple excision of the mass without any recurrence during the follow-up period.
The clinical, sonographic, and histological data of our report may help clinicians who are confronted by various kinds of analogous facial lesions to decide the proper management for their patients.
Notes
No potential conflict of interest relevant to this article was reported