INTRODUCTION
Cutaneous horns are cornified projections resembling the horns of animals. Although these lesions can be found anywhere, the face and scalp account for 30% of all occurences. They are attributable to an array of benign (61.1%), premalignant (23.2%), and malignant (15.7%) lesions [1]. Reported herein are two elderly women, each treated for a facial cutaneous horn. Histopathologic examinations confirmed actinic keratosis and squamous cell carcinoma as underlying lesions.
CASE REPORT
Case 1
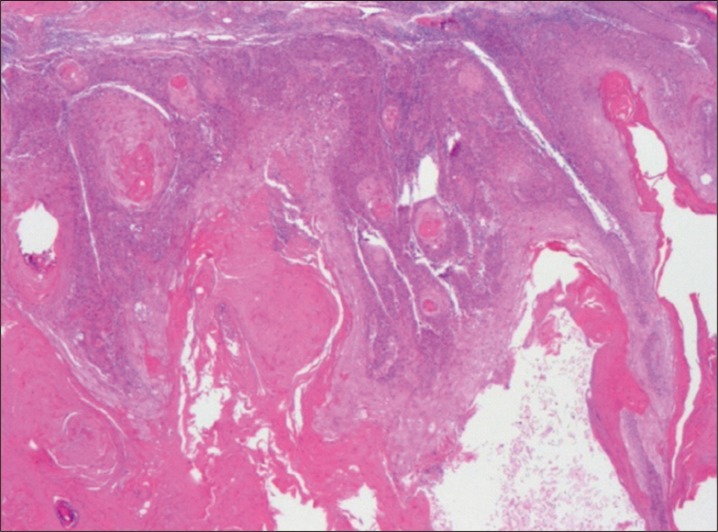
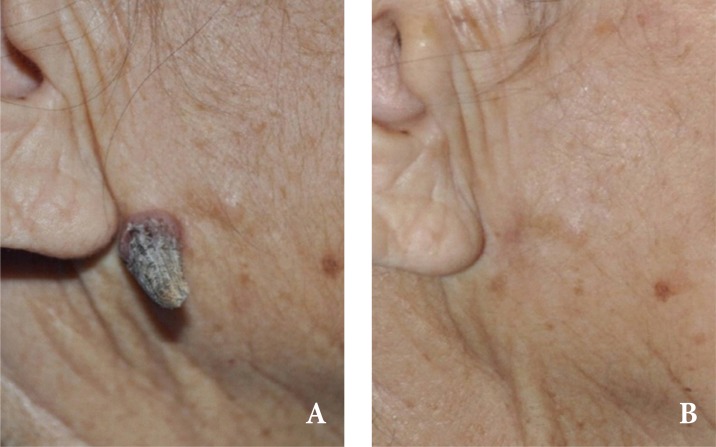
An 81-year-old woman presented with a nasal skin lesion, which she first noticed 8 months ago. Prior trauma or surgery was excluded by history. Physical examination revealed a 1.5 cm, firm arciform projection with a broad but nonerythematous base at bridge of nose (Fig. 1A). The lesion was excised under local anesthesia to include a 3.0-mm margin. The resulting defect was closed with local advancement of undermined skin flaps from both sides (Fig. 1B). Histologically, a thick cornified mound was prominent, with focal parakeratosis. Within the Malpighian layer, keratinocytes showed variable loss of polarity and disarray, while bundles of dermal collagen rested horizontally. Because of this features, the lesion was diagnosed as actinic keratosis (Fig. 2). The wound healed well postoperatively, and no recurrence was observed for the 2 months of follow up period.
Case 2
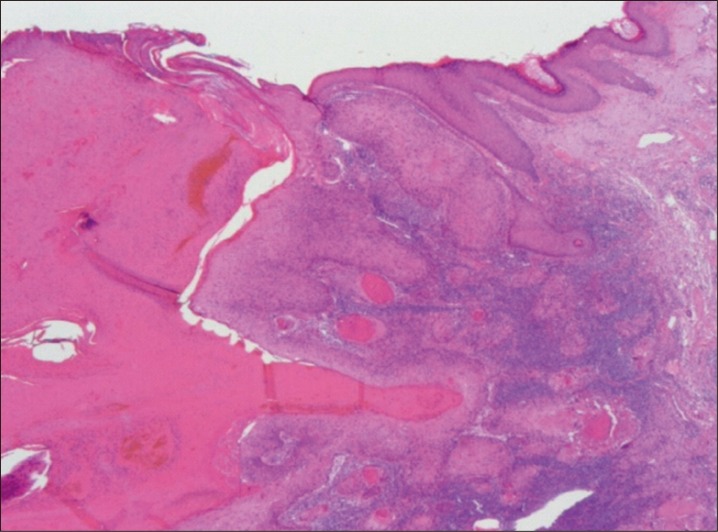
A healthy 86-year-old woman presented with an asymptomatic right preauricular lesion of 3-month duration. The lesion had appeared spontaneously and was unrelated to trauma. On physical examination, a 1.8-cm tall cutaneous horn was present in the right preauricular area, with erythema at the base (Fig. 3A). Excisional biopsy was revealed the lesion to be consistent with squamous cell carcinoma (Fig. 4). The patient did not have any lymphadenopathy, and subsequently underwent definitive resection with primary closure of the defect (Fig. 3B). No residual malignancy was evident in histologic sections. The wound healed without complications, and the patient was free of local recurrence at 8 weeks post operation.
DISCUSSION
Cutaneous horns are conical cutaneous projections consisting of densely compacted keratin. They may range in size from a few millimeters to several centimeters. Although any anatomic site may be affected, sun-exposed skin is primarily at risk. Face and scalp account for 30% of all such lesions, the underpinnings of which may be benign or malignant. Fair-skinned patients 50 years or older are most susceptible [2]. There is no real gender predilection, but the likelihood of associated malignancy is greater in men (versus comparably aged women) [3]. Those arising in malignancies tend to more painful and erythematous [4]. Broader-based lesions also are more often linked with premalignancy or malignancy [5].
The pathogenesis of cutaneous horn is not fully understood. The horn itself is cornified debris that is of no clinical consequence. It is the underlying, albeit largely benign, pathology that is the primary concern [6] and impetus for this report. An array of benign lesions (seborrheic keratosis, viral warts, keratoacanthoma, trichilemmoma, epithelial hyperplasia, and more), premalignant conditions (actinic keratosis, arsenical keratosis, and Bowen's disease), and malignancies (squamous cell carcinoma, basal cell carcinoma, metastatic renal carcinoma, granular cell tumor, sebaceous carcinoma, and Kaposi's sarcoma) may be associated with cutaneous horns. Generally, these lesions present as isolated projections, arising in conjunction with actinic keratosis [5,7].
Despite the fact most of the cutaneous horns themselves are benign, a recent study indicates that 39% of cutaneous horns are manifestations of malignant or pre-malignant disease [3]. Patients who worked as farmers, with a lifetime history of sun exposure, were inclined to develop actinic keratoses and squamous cell carcinomas. Actinic keratosis is a premalignant lesion that starts as a flat scaly patch, later developing into a large wart-like growth. It may range from 2ŌĆō6 mm in size and vary in color (tan, pink, red, dark, light, or a combination of shades). Sun-exposed areas of the body are common locations. Actinic keratoses may progress to squamous cell carcinoma [8].
Treatment options include wide surgical excision, CO2/Nd-YAG laser, and electrocautery. Cryotheraphy may be used alternatively but is not recommended, given that histopathologic examination is then precluded. Deep biopsy or total excision is the favored approach, ensuring that the base of the horn will be visible in histologic preparations [9]. Frozen section should be considered in large, erythematous, or painful lesions or if long-term sun exposure is documented by history.
Histopathologic assessment of disease at the base of horn is strongly recommended and is essential in the elderly, checking for potential malignancy. Excision with primary repair will suffice for clinically innocuous lesions where patient history is not alarming. Otherwise, wide surgical excision with adequate uninvolved margins and perhaps frozen section may be done to avoid further surgical intervention. If malignancy is diagnosed, lymph nodes draining the site must be evaluated to rule out metastasis.