INTRODUCTION
The incidence of oral cavity cancer and oropharyngeal cancer is increasing in Korea, with 11,792 cases occurring between 2008 and 2012 and 7,484 cases occurring between 1996 and 2000. In the year 2012, oral cavity and oropharyngeal cancer was diagnosed in 2913 patients, whose 5-year survival rate was at 62.2% (survival rate for all cancers combined at approximately 68%) [1].
The oral cavity space extends from the skin-vermilion junctions of the lips to the junction of the hard and soft palates above and to the line of circumvallate papillae below to include the lip, anterior two-thirds of the tongue, buccal mucosa, floor of the mouth, upper and lower gingiva, retromolar trigone, and hard palate. The oropharyngeal space is located between the soft palate superiorly and the hyoid bone inferiorly and is divided into the base of the tongue, tonsillar region, soft palate, uvula, and posterior and lateral pharyngeal walls [2].
In addition to tobacco and alcohol use as major risk factors, the development of oral and oropharyngeal cancers (OPCs) have been shown to correlate with ultraviolet radiation, human papillomavirus (HPV), immunosuppression, the areca nut, and lower socioeconomic status. While consumption and alcohol and tobacco products have been decreasing or remains constant, the incidence of OPC continues to increase because of the increasing incidence of the HPV-associated tumors, which is prevalent in young adults with minimal tobacco and alcohol exposure [3].
ORAL CAVITY CANCER
The oral cavity is a common site of malignancy worldwide and is especially common in developing countries [4,5]. Squamous cell carcinoma represents the most common histologic type, with tobacco and alcohol use being the primary etiologic factors [6]. Although oral cancer can be detected early, patients frequently present in advanced stages. The treatment of choice is surgical resection with or without postoperative adjuvant chemotherapy and/or radiotherapy. Advancements in surgical resection and the addition of adjuvant therapies have led to improved survival rates over the past decade [7]. This success in multidisciplinary approach stems from basic strategies to maximize disease control and to preserve the natural form and functions of the oral cavity.
OROPHARYNGEAL CANCER
Located posterior to the oral cavity and between the nasopharynx and larynx, the oropharynx aids in critical functions such as swallowing and maintaining patent airway. The oropharynx is also crucial for speech because of the need for mobility and pliability and because of proximity of the base of tongue to the larynx. The oropharynx consist of the soft palate, posterior and lateral pharyngeal walls, faucial arches, tonsillar fossa, and the base of tongue. Anatomically, the non-restraining soft tissue boundaries as well as the rich lymphatic supply allow for escape of malignant cells, which results in most patients presenting with advanced disease (stage III or IV) [5]. Traditionally, the oropharynx was considered to be difficult to access by surgical means, and refinement of radiation therapy and the use of combination chemoradiotherapy have made nonsurgical approaches the standard practice [8]. However, recent advancements in minimally invasive techniques have rekindled interest in surgical management of oropharyngeal cancers.
TREATMENT OF OROPHARYNGEAL CANCERS
Oropharyngeal cancers are generally treated by a combination of surgery, radiotherapy, and/or chemotherapy. The treatment protocol is dependent on tumor size, site of occurrence, staging, the medical and nutritional status of the patient, and patient preference for treatment modality [9]. Both the tumor and its treatment can interfere with speech and swallowing function, which can subsequently interfere with quality of life and ability to work. As such, the treatment of oropharyngeal cancers should aim to preserve function and to minimize complications, in addition to curing the disease itself. A comprehensive multidisciplinary team should include the coordination of oncologic and plastic surgeons, medical oncologist, radiation oncologist, oral health care providers, nutritionist, nurse specialist, and speech pathologist.
FREE FLAP RECONSTRUCTION OF ORAL AND OROPHARYNGEAL DEFECTS
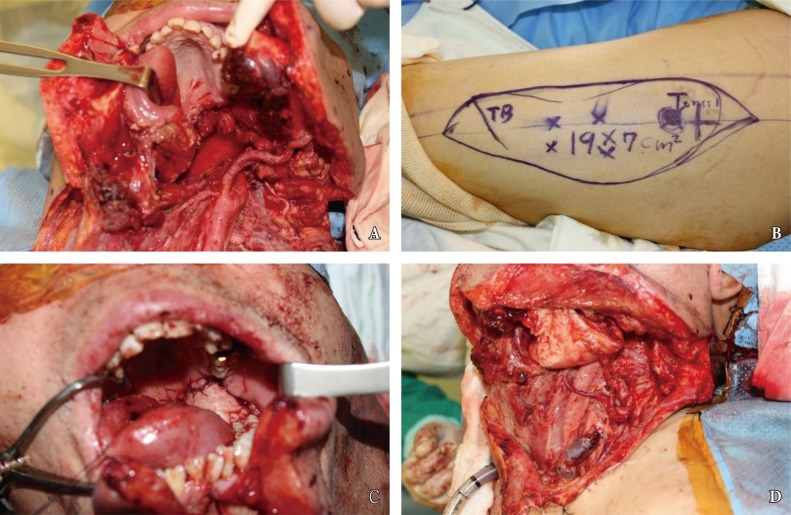
Extensive surgical resection of the aerodigestive track can result in a large and complex defect of the oropharynx, which represents a significant reconstructive challenge for the plastic surgery. Development of microsurgical techniques has allowed for free flap reconstruction of oropharyngeal defects, with superior outcomes as well as decreases in postoperative complications, as compared to non-free flap reconstructive options [10]. With regard to the type of free flaps used in oropharyngeal reconstruction, fasciocutenous free flaps and enteric free flaps such as jejunum are widely used. However, enteric free flaps lead to frequent dysphagia necessitating laparotomy [11]. Fasciocutaneous flaps include the radial forearm free flap and anterolateral thigh free flap, and these flaps are associated with excellent functional outcomes and low donorsite morbidity (Fig. 1).
FUNCTIONAL OUTCOMES FOLLOWING COMPLEX OROPHARYNGEAL RECONSTRUCTION
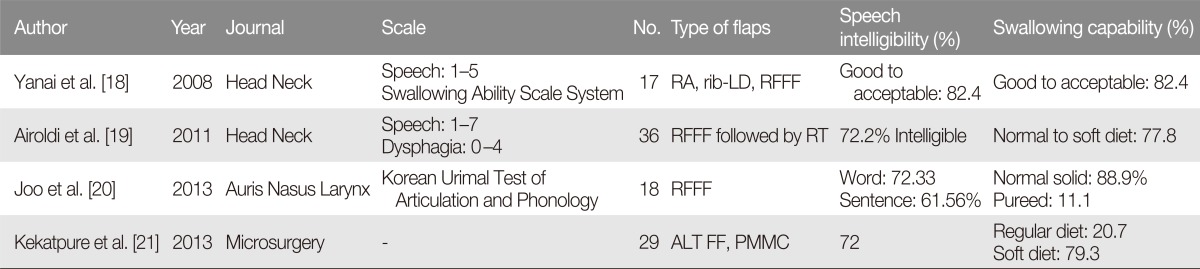
The reconstructive goals for oral and oropharyngeal defects are to restore the anatomy, to maintain continuity of the intraoral surface and oropharynx, to protect vital structures such as carotid arteries, to cover exposed portions of internal organs in preparation for adjuvant radiation, and to preserve complex functions of the oral cavity and oropharynx [12,13,14]. With the development of microsurgical techniques, free flaps has become the most popular choice for reconstruction of oral and oropharyngeal defects in most hospitals, with flap survival rates reported to be as high as 95% [15,16,17]. Because the important functions of oral cavity and oropharynx, the purpose of reconstruction has focused on preserving such functions and helping patients to achieve a normal life (Table 1) [18,19,20,21]. Postoperative recovery of these functions is related to preservation of the anatomic structures and dimension of the oropharyngeal space [22,23,24,25]. A variety of insetting procedures have been developed with respect to minimizing functional deficits (e.g., folded or deepithelializing flaps). However, flap insetting remains a challenging problem for reconstruction surgeons.
ANASTOMOSIS LEAK
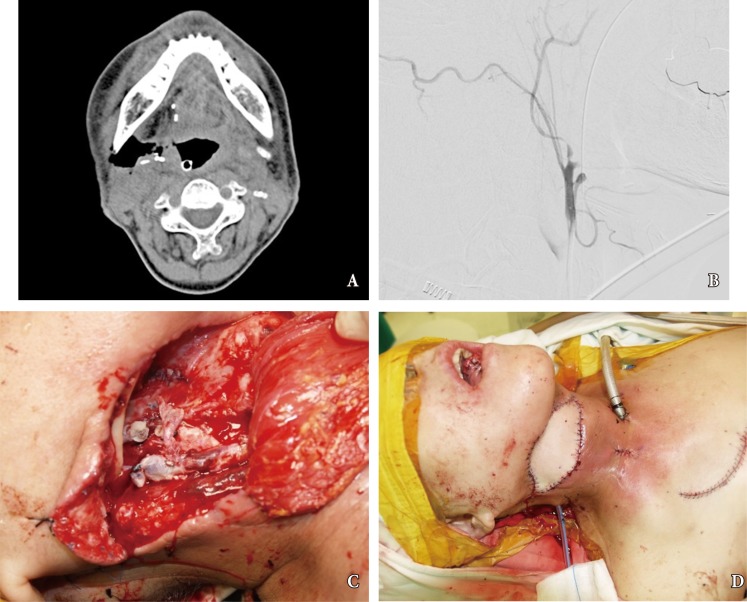
Despite advancements in oral reconstructive techniques, fistulas around the flap margin is the most common and serious complication, occurring in 9% to 23% of cases [26]. Fistulas can further result in secondary complications such as salivary leakage, delays in postoperative chemotherapy and radiotherapy, and even carotid blowout syndrome (CBS) (Fig. 2). The latter complication, CBS, is caused by the tumor mass compromising the vascular axis or leakage of saliva, and results in rupture of the carotid artery which can lead to a lethal episode of hemorrhage. Fistulous tract from oral cavity into the connective tissue allows introduction of saliva, which is laden with bacteria and damages to the outer lining of the arterial wall [27]. The risk of anastomotic leak should be minimized with proper choice of suture material, tension-free insetting, and dead space obliteration. Fistula rates are similar in partial and circumferential reconstructions, and proximal fistulas are rare with the anterolateral flap. Incidence of fistula formation is higher with the radial forearm flap along the longitudinal seam of the tubed fasciocutaneous f lap. Any questionable tissue should be resected until only well-vascularized tissue is observed in the proximal pharynx and cervical esophagus. The flap-to-wound margin should be closed by a single layer of simple interrupted sutures. The skin and mucosal edges should be inverted into the lumen, with suture 5ŌĆō7 mm apart from each other.
DONOR-SITE MORBIDITY
Fasciocutaneous free flaps have been used for oral and oropharyngeal reconstruction since 1981 [28]. While the reconstructive features are outstanding for flaps such as forearm free flaps, donor-site morbidity remains unsatisfactory, especially when split-thickness skin graft is required [29]. Donor-site morbidity for such flaps are reported for up to 53% of cases and include tendon exposure, delayed healing, reoperation, tendon adhesion, limitation of joint movement, and poor cosmesis [30]. Changing the flap design for a proximal site along the forearm or suprafascial elevation can be useful for decreasing morbidity, donor site pain and scarring [31]. Recent studies have reported improved outcomes for donor-site morbidity by employing dermal substitutes, tissue expander, local flap with rotation, and full thickness skin grafts (Fig. 3) [32,33,34].