Sinus Tract Formation with Chronic Inflammatory Cystic Mass after Beta Tricalcium Phosphate Insertion
Article information
Abstract
Beta tricalcium phosphate (β-TCP) is one of allogenic bone substitute which is known to have interconnected pores that draws cell and nutrients for bone generation. It has been resulted in good outcomes for bone defect coverage or augmentation. However, several studies have also reported negative outcomes and associated complications including unexpected formation of cystic mass, continuous pain and secretion. We present the case of a 36-year-old man with a right cheek cystic mass who had a history of right zygomaticomaxillary (ZM) complex fracture and surgical correction with β-TCP powder insertion to ZM bone defect. Excisional biopsy under local anesthesia revealed calcified mass in a sinus tract which was found to be connected to the ZM bone defect site in postoperative computed tomography image. Further excision under general anesthesia was performed to remove the sinus tract and fine granules which filled the original defect site. Pathologic report revealed bony spicules and calcification materials with chronic foreign body reaction. Postoperative complications and recurrence were not reported.
INTRODUCTION
Allogenic bone substitutes that replace autogenous bone grafts, should be biocompatible, non-antigenic, and degradable with osteogenic capacity, and are constant pursuits in maxillofacial surgery [12]. Beta tricalcium phosphate (β-TCP) is one such biomaterial. Although good outcomes have been reported for bone defect coverage or bone augmentation [2345], several studies have also reported negative results when filling bone defects with β-TCP, including poor bone formation, unexpected formation of cystic mass, continuous pain, and secretions, which may attribute to soft tissue inflammation after insertion of β-TCP [1,678]. We present the case of a 36-year-old man with a right cheek cystic mass who had a history of right zygomaticomaxillary (ZM) complex fracture and surgical correction with β-TCP powder insertion. The mass was initially believed to be an epidermal cyst, but histologically demonstrated calcified clusters and bony spicules, which may be due to the failure of β-TCP bone formation.
CASE REPORT
A 36-year-old man visited our department with a mass on his right cheek, measuring 1×1 cm lateral to the oral commissure. He had undergone surgical correction for right ZM complex fracture with bone defect at ZM buttress and right inferior orbital wall fracture due to road traffic accident 6 years prior. The bone defect was filled with β-TCP bioceramic powder (PolyBone, Kyungwon Medical Co. Ltd., Seoul, Korea). The mass had appeared 5 years prior along with signs of inflammation of the adjacent skin, such as redness and tenderness (Fig. 1). Initially, excisional biopsy through direct skin incision under local anesthesia was performed with a preliminary diagnosis of infected epidermal cyst. However, the mass was calcified and had a sinus tract (Fig. 2). The tract was not completely removed as it extended into the deep tissue. Biopsy results revealed chronic inflammation around the calcified fragments. Computed tomography (CT) with contrast enhancement revealed that the sinus tract was connected to the ZM bone defect site (Fig. 3). Bone formation was not seen at the defect site and remnant calcified granules were found above the defect.

The mass on the right cheek with inflammatory signs. Preoperative photography.
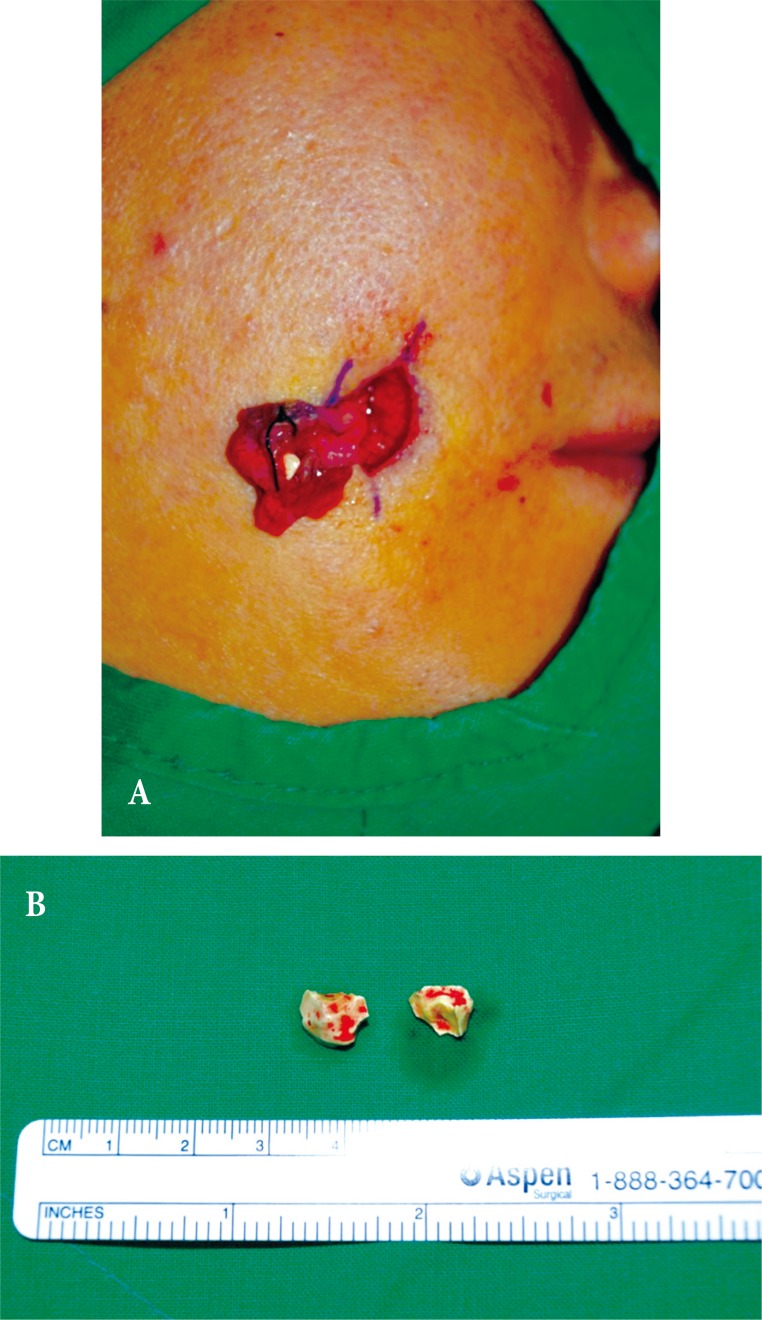
(A) Excised sinus and calcified fragments at first operation. (B) Calcified masses removed.
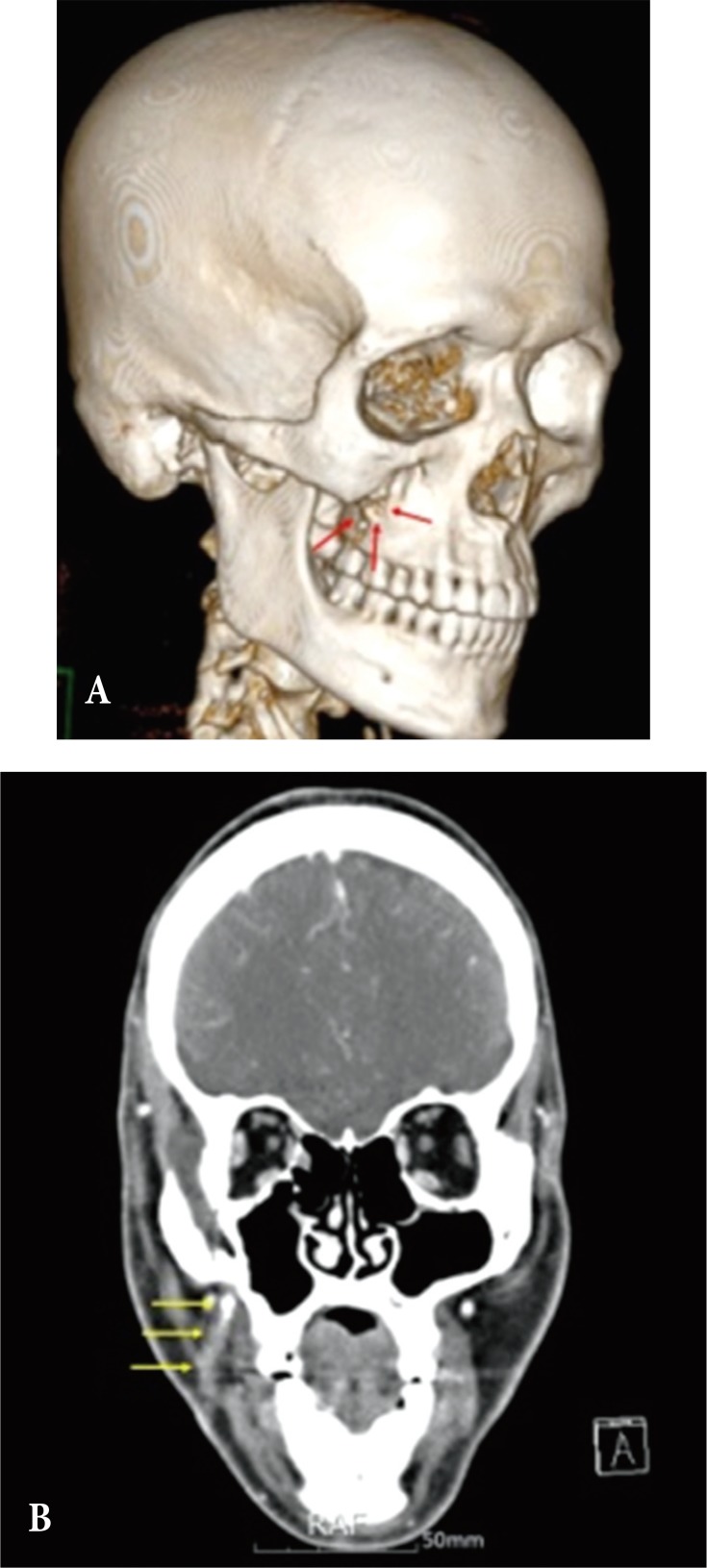
(A) Zygomaticomaxillary buttress defect (red arrows) was shown. (B) Computed tomography with contrast enhancement revealed that the sinus tract (yellow arrows) was connected to the defect site.
Further surgical resection under general anesthesia was performed to remove the sinus tract and remnant granules completely. Intraoral approach with right upper buccogingival incision was used to reveal the fibrous sinus tract connecting the defect to the subcutaneous tissue. The tract was excised from the superficial fat tissue, and resected in an en bloc pattern with the help of a guide probe (Fig. 4). Dense adhesive tissue at the defect was also completely removed and curettage of the fine granules filling the ZM defect was performed with copious saline irrigation. The fine granules were connected to skin through the sinus and covered by a cystic wall, which isolated it from the adjacent bony structures. The Stensen's duct was intact. Histopathological examination revealed that it was a foreign body reaction with chronic inflammation of the sinus tract and that the tiny granule was degenerated bony spicules and calcification materials (Fig. 5). The surgical wound healed without any complication and no recurrence was noted.

(A) Buccogingival approach revealing fibrous sinus. (B) Excised sinus with probe guide at second operation.

(A) Multiple infiltrated lymphocytes were shown (H&E, ×100). (B) Some calcified materials (red arrows) were confirmed that causing foreign body reaction (H&E, ×200).
DISCUSSION
The maxillary bone is related to facial aesthesis and several oral functions such as speech, swallowing, and mastication. It supports the orbital structures, and separates the oral and orbital cavities [9]. Autogenous bone graft is considered the material of choice for the reconstruction of bone in maxillofacial surgery [1]. However, to prevent secondary donor site morbidity and increased duration of the operation for the harvesting procedures, several artificial bone substitutes, including bioceramics, allograft bone matrix, and composites have been developed for craniofacial defects [4].
The major inorganic component of bone tissue is hydroxyapatite (HA), and many different calcium phosphate ceramics have been utilized as a material for bone substitutes. As a bone substitute, HA is highly osteocompatible and expresses sufficient osteoconductivity, but stoichiometric HA is unbioresorbable, and has much less mechanical strength than bone tissue because there is no organic component such as type I collagen in the bone substitute. Therefore, the HA that remains in bone tissue can cause serious clinical problems [10].
β-TCP is a bioceramic material and is known to have interconnected pores that create a capillary force to draw cells and nutrients into the material for bone generation [2]. It resolves completely in the human body in a centripetal pattern followed by new bone formation [46], so has used as most popular bioresorbable materials for bone substitutes. β-TCP, alone or mixed with other bioceramics, has been reported to have favorable outcomes in maxillary sinus augmentation for dental implant fixation and reconstruction of the orbital floor and bone defects followed by bone tumor resection and curettage [2345].
Adverse effects of β-TCP have also been reported. Poor osteogenic effect has been observed in several in vivo studies [268]. Friesenbichler showed that bone defects covered with β-TCP mixed with calcium sulfate could result in soft tissue inflammation leading to delayed wound healing, continuous wound secretion and pain, and formation of cysts [7]. In this case, follow up CT revealed bone defect in the right ZM buttress area implying failure of bone formation and that calcified fragments and bony spicules were located away from fracture site, in a sinus connected to the defect site. Histologically, chronic foreign body reaction was found even 6 years after insertion of β-TCP. Foreign body reaction is a response of wound healing following the insertion of biomaterials and it may play a major role in the formation of bony spicules, calcified clusters, and sinuses [11011]. de Souza et al. reported foreign body reaction and inflammatory infiltrates in β-TCP insertion sites; they hypothesized that it may lead to expulsion of β-TCP clusters from the original defect site [1]. Sinus formation resulting from foreign body reaction was also reported [12].
In conclusion, because of the debatable findings regarding β-TCP demonstrated in our case and several other studies, informed consent is very important when filling maxillofacial defects with β-TCP about the possibility of failure of bone formation along with formation of cysts and inflammatory complications, including pain, delayed wound healing, continuous discharge, and sinus formation. Additionally, long-term follow up with radiographic examination including X-ray and CT is needed for evaluating bone formation.
Notes
CONFLICT OF INTEREST: No potential conflict of interest relevant to this article was reported.
PATIENT CONSENT: The patient provided written informed consent for the publication and the use of their images.