INTRODUCTION
Rhabdomyomatous mesenchymal hamartoma is a congenital skin mass which was first described as a mesenchymal hamartoma with striated muscle in 1986 [1]. Since its first report, 66 more cases have been reported in the literature [2]. It is dermal and subcutaneous lesion which exhibit an abnormal arrangement of mesenchymal elements and prominence of skeletal muscle. It's histologic feature is different from similar masses such as fetal rhabdomyoma, superficialis lipomatosus, fibrous hamartoma of infancy and neuromuscular hamartoma [1]. Most lesions were observed on the head and neck, but some cases were appeared on the sacral area, tongue, vagina and great toe [3]. We report here a case of Korean patient of rhabdomyomatous mesenchymal hamartoma on the midline of chin.
CASE REPORT
A 17-month-old boy was seen in the pediatric plastic and reconstructive surgery clinic of this hospital because of a mass on his chin. His parents wanted to remove it. They explained that it had been observed since his birth and there was no acute size change. They also complained that the boy frequently touches his mass.
His height was 80 cm (25–50 percentile) and weight was 10.7 kg (25–50 percentile). On his chin, there was a round, protruding soft tissue mass located at midline and tip of his chin. The measured size of the mass in the clinic was 0.7×0.7 cm. It had a skin-tone color but slightly pinkish on its top surface. It did not have an opening on its surface and there was no discharge from it. Also the skin around the mass did not show an inflammatory sign-redness, swelling or heat (Fig. 1). Preoperative ultrasound sonography was conducted to evaluate the mass (Fig. 2). 0.84×0.34 cm hypoechoic mass was located at the subcutaneous level. The possibility of malignancy such as rhabdomyosarcoma was low because the patient had showed no symptoms suggesting malignancy-such as rapidly enlarging mass or 4 palpable lymph node [4]. So without pathological analysis, primary excision of the mass was planned.
The operation was done under the general anaesthesia. The patient was laid in a supine position. Elliptical incision line was designed around the mass to excise the mass along the relaxed skin tension line. Skin incision was made along the line. After subcutaneous dissection, a stalk-like structure was found which was projected from the mass and penetrate the mentalis muscle. It was inserted to the periosteal tissue below the muscle. The stalk was skeletonized with meticulous dissection and resected at its most proximal end to leave the tissue at least (Fig. 3). The muscle and subcutaneous tissue were repaired each with vicryl 5-0. The skin was closed primarily with prolene 6-0. An ointment (Tarivid) was applied on the wound. The wound was covered with Medifoam. After 6 days, the stitches on the skin were removed. There were no postoperative complications such as wound dehiscence or infection.
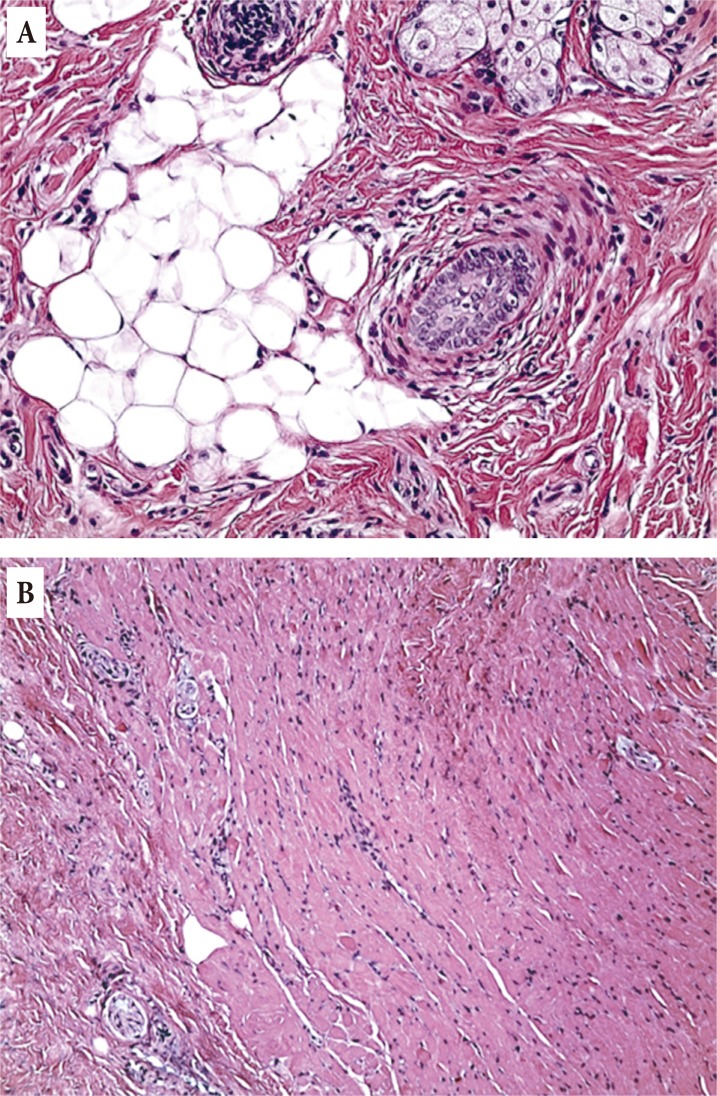
Histological analysis was asked to our pathologist. On their report, fibroepithelial lesion with increased mature skeletal muscle and peripheral nerve fibers were observed in the tissue (Fig. 4). Adipose tissue, intermingled collagen fibers were also present. The pathological diagnosis was rhabdomyomatous mesenchymal hamartoma.
DISCUSSION
Rhabdomyomatous mesenchymal hamartoma is a rare congenital skin mass which is a disordered mixture of striated muscle, adipose tissue and collagen fiber [5]. It is a lesion of the deep dermis and subcutaneous tissue composed of mature skeletal muscle fibers intermixed with skin adnexa, such as sebaceous glands, hair follicles and sweat glands. These lesions may also include adipose tissue, nerves, blood vessels and collagen. 66 cases of rhabdomyomatous mesenchymal hamartoma have been reported until 2016. It has showed a slight male predominance [3].
Rhabdomyomatous mesenchymal hamartoma presents as singular or multiple dome-shaped or pedunculated masses [6]. It usually present at the midline of the head and neck region. The nose and chin are the most common sites, followed by the anterior side of the neck, periorbital, perioral, and preauricular regions. But other cases have also been reported on the tongue, perianal region, vagina, and great toe [4]. Some lesions were in association with other congenital abnormalities (e.g., cleft lip and/or palate) or neurocutaneous syndromes [3].
Rhabdomyomatous mesenchymal hamartoma has been associated with oculocerebrocutaneous (Delleman) syndrome, a rare condition accompanied by orbital cysts, cerebral malformations, and focal skin defects [7]. Also rhabdomyomatous mesenchymal hamartoma can present as skin mass as part of Goldenhar syndrome, which is represented by craniofacial and central nervous system anomalies-microtia, colobomas, facial asymmetry, absence of the corpus callosum, and skin tags [8].
The differential diagnosis for midline chin rhabdomyomatous mesenchymal hamartoma includes dermoid cyst, glioma, lipomatous nevus (superficialis lipomatosus), skin tag, fetal rhabdomyoma, fibrous hamartoma of infancy and neuromuscular hamartoma (benign Triton tumor), embryonal rhabdomyosarcoma [1]. Fetal rhabdomyoma, neuromuscular hamartoma, embryonal rhabdomyosarcoma, and rhabdomyomatous mesenchymal hamartoma all contain skeletal elements in the dermis and/or subcutaneous tissue. However, in rhabdomyomatous mesenchymal hamartoma, the striated muscle is well differentiated and randomly arranged with adnexal structures, blood vessels and peripheral nerves [2]. In fetal rhabdomyoma, there are less differentiated and denser muscular elements. And in neuromuscular hamartoma, the muscle fibers are intimately associated with nerve fibers [4]. Embryonal rhabdomyosarcoma has a malignant histologic characteristics exhibiting an abnormal arrangement of dermal mesenchymal elements and prominence of skeletal muscle. So it's significantly different from rhabdomyomatous mesenchymal hamartoma.
Rhabdomyomatous mesenchymal hamartoma is a benign tumor since there were no reported cases of malignant transformation [9]. So, the treatment of rhabdomyomatous mesenchymal hamartoma is a simple excision. There were no reported recurrences after excision [4]. Even without excision, two cases has been reported which were spontaneously regressed [3,8].
To the best of our knowledge, there were only two adult cases [7,10] of rhabdomyomatous mesenchymal hamartoma and two pediatric cases [11,12] in Korea. Among the pediatric cases, one patient was 7-year old boy who represented a vestibular rhabdomyomatous mesenchymal hamartoma after a trauma on his nose. Another case was newborn female infant who had a vaginal rhabdomyomatous mesenchymal hamartoma. So this is the first case of congenital rhabdomyomatous mesenchymal hamartoma in Korea represented as a chin mass at midline.