Modified Abbé flap for reconstruction of Cupid’s bow and vermilion tubercle in secondary cleft lip deformity
Article information
Abstract
Background
Abbé flap technique is one of the most challenging operations to correct horizontal deficiencies in secondary cleft lip deformity. Since its first introduction, the operative method was dynamically modified from simple variation to complete conceptual change, but conventional Abbé flap has many drawbacks in esthetic and functional aspect. Our purpose was reconstructing the symmetry of Cupid’s bow and central vermilion tubercle with minimal sequalae.
Methods
From 2008 to 2016, this technique was applied to 16 secondary cleft lip patients who had total or more than 60% of unilateral deficiency of Cupid’s bow and central lip or tubercle pouting deficiency. A quadrangular-shaped flap was transferred from vermilion including skin and white line of central or contralateral lower lip. Pedicle division and insetting were made at 9 (unilateral) or 10 (bilateral) days after transfer. Secondary lip revision was done with open rhinoplasty after wound maturation.
Results
Overall satisfaction was high with modified technique. Scar was minimally noticeable on both upper and lower lip especially. Balanced Cupid’s bow and symmetric vermilion tubercle were made with relatively small size of flap compared to conventional Abbé flap. An accompanying benefit was reduced ectropion of lower lip, which made balanced upper and lower lip protrusion with more favorable profile.
Conclusion
A new modified Abbé flap technique showed great satisfaction. It is worth considering in secondary cleft lip patient who has central lip shortage and asymmetry of upper lip vermilion border line. Our technique is one of the substitutes for correction of horizontal and central lip deficiency with asymmetric Cupid’s bow.
INTRODUCTION
In secondary cleft lip deformities, tight upper lip, absent or asymmetric Cupid’s bow, central lip and tubercle pouting deficiency are not treated efficiently with simple revision surgery [1]. The Cupid’ bow and central tubercle are a cardinal structures for symmetric upper lip [2]. They do not provide simple solution for lack of upper lip tissue and structural restoration. The concept of brining lower lip tissue into insufficient upper lip has long been introduced almost 200 years before, which was described by Robert Abbé, so-called “lip switch flap” in 1898 [3]. This technique became one of the most challenging operations in secondary cleft lip surgery. Conventional Abbé flap requires long incision and bulky tissue, which led to many drawbacks such as long and newly additional scar on both upper and lower lips [4]. A long while, many authors have contemplated to modify the Abbé flap to improve the results [5-9]. We would like to introduce a novel method to reconstruct the symmetry of Cupid’s bow and central tubercle with minimal sequalae.
METHODS
From 2008 to 2016, this technique was applied to 16 patients who had total or more than 60% of unilateral deficiency of Cupid’s bow and central lip or tubercle pouting deficiency in those of patients with secondary cleft lip deformities. The surgeries were conducted by single surgeon (C.K.L.). The basic demographics such as diagnosis, age, sex, short of Cupid’s bow, and flap size are documented. Preoperative measuring included the length and peak-point level of Cupid’s bow in normal and cleft side. The shortage of length and size of the transferring tissue was carefully contemplated and documented as well (Tables 1, 2). The medical records and patient response were investigated. The operator and another plastic surgeon were participated in evaluation of outcome by any methods such as direct inspection, subjective satisfaction and clinical photographs, using visual analogue scale (VAS) graded from 0 (worst outcome) to 10 (best outcome) before and after the surgery. Interobserver consistency was measured with Cronbach’s α and analyzed with IBM SPSS ver. 22.0 (IBM Corp., Armonk, NY, US). Statistical significance was defined when p-value was less than 0.05.
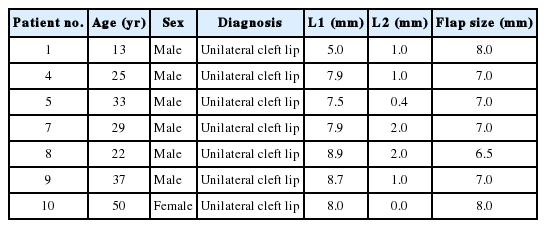
Patient demographics of unilateral cleft lip

Patient demographics of bilateral cleft lip
Operative technique
Unilateral cleft lip deformity
Under either general or local anesthesia, the patient was supine position with mild neck extension. The full face was prepared in usual sterile manner. Operative design was made differently in terms of shape and location according to the diagnosis of the patient, whether it was bilateral or unilateral cases (Fig. 1). The local injection was made with 1% lidocaine and 1:200,000 epinephrine solutions at the recipient and donor site. The eccentric previous surgical scar was resected to keep up the symmetric slant with normal vermilion border line as same manner (Fig. 1B, C). The defect was widened by splitting and meticulous trimming of scar tissue inch by inch even though normal tissue, which released from tightness of upper lip partially. The proper recipient space was made as equal size of flap which being a same length of normal vermilion border line including remaining length.
Overall design of the modified Abbé flap for Cupid’s bow reconstruction in bilateral cleft lip deformity (A), left side (B) and right side of lip (C) in unilateral cleft lip deformity. Scar tissue to be excised and released (a), flap to be transferred and inset (b) and area to be discarded or deepithelialized, for primary closure of the donor site (white-dotted area).
A pentagonal-shaped flap was designed as 6 to 10 mm-wide vermilion including 2 mm-high skin and white line from central or contralateral side of lower lip (Fig. 1). Donor site was closed primarily, in which the scar was not over the labiomental sulcus. After confirmation of intact blood flow, the medial-based labial artery pedicled flap was transferred to clockwise or counterclockwise fashion to recipient site. The triangular part of the distal tip of the flap was discarded or deepithelialized and inserted into ready-made space of upper lip. The flap was closed layer by layer in order of mucosa, muscle, subcuticular layer and skin (Fig. 2A, B). Pedicle division and flap insetting were made 9 days after the initial surgery under local anesthesia after conformation flap viability by pedicle ligation for 30 minutes. Further lip revision combined with open rhinoplasty was done after wound maturation for more aesthetic outcome.
Intraoperative clinical photographs of Abbé flap design with flap transfer (A, B; case 15), before Abbé flap and 2 years after the flap transfer including open rhinoplasty and two stages of scar revision (C, D), and preoperative and postoperative appearance (2 years) of lip protrusion and profile (E, F).
Bilateral cleft lip deformity
The overall procedures were similar to the operation in unilateral cleft lip patient. The difference was the location and size of flap which was from center of lower lip from 7 to 10 mm in width (Fig. 1A). The recipient site was prepared by excision of tiny tissue including midline notching scar. The gap was enlarged by splitting and meticulous trimming to make same space with flap size. If the Cupid’s bow was normal ranged state, the disfigured and notched vermilion mucosa was excised only. Then, the flap was transferred from mucosal part of lower lip vermilion without white line and skin. Pedicle division and flap insetting were made 10 days after the initial surgery.
RESULTS
Mean patient age was 26.5 years (range, 13 to 50 years); 13 were males and three were females. There were nine bilateral cleft lip and seven unilateral cleft lip patients. Overall satisfaction was high with modified Abbé flap operation in terms of shape and symmetry. Scar was barely noticeable. However, the color of vermilion mucosa takes a long time to similar with on site color of upper lip mucosa. Most of the patient showed balanced Cupid’s bow and relatively symmetric vermilion border line. Some patients were revised of scar and convolutional vermilion line. An accompanying benefit was reduced ectropion of lower lip, which made balanced upper and lower lip protrusion and favorable profile (Figs. 2-5). There was no acute complication regarding operation site. The median VAS score was 4 (range, 3 to 5) in bilateral cleft lip patients and 5 (range, 3 to 6) in unilateral cleft lip patients preoperatively, and 7 (range, 5 to 8) in bilateral cleft lip patients and 6 (range, 5 to 8) in unilateral cleft lip patients postoperatively from one observer. The other observer found the same results, while the median VAS score was 7 (range, 5 to 8) in bilateral cleft lip patients. Interobserver consistency was high in both pre operative and post operative evaluation (Cronbach’s α=0.831, p =0.001 preoperatively and Cronbach’s α=0.803, p =0.002 postoperatively).
Preoperative (A) and postoperative (B) clinical photos of Cupid’s bow reconstruction (case 1) and lip protrusion and profile (C, D). Postoperative photos were taken just before any revisions, 6 months after Abbé flap.
Preoperative (A) and postoperative (4 years, B) clinical photos of Cupid’s bow reconstruction (case 14) and lip protrusion and profile (C, D). The patient underwent lip reduction, open rhinoplasty, and four rounds of laser treatment.

Preoperative (A) and postoperative (B) clinical photos of left Cupid’s bow reconstruction (case 3). Postoperative photos were taken just before any revisions, 6 months after Abbé flap.
DISCUSSION
Abbé flap technique was modified dynamically since its first introduction in 1898 [3]. Our technique is unique in its conception, design and flap size. Minimal lip tissue is transferred for less morbidity and minimal scar, but a small part of vermilion border line and skin is essential for making Cupid’s bow which is disfigured or absent in almost all secondary cleft lip deformity patients. The lower lip is the only substitutive source for upper lip which severely disfigured vermillion border line or short of Cupid’s bow. Unilateral cleft lip deformity has short of Cupid’s bow in cleft side over 90% of patient in our experience. The flap must be transferred from contralateral side of lower lip for restoration of vermilion border line gradient. In bilateral cleft lip deformity, the Cupid’s bow was substituted totally for symmetry. The middle segment of lower lip presents an excellent substitute for Cupid’s bow. In unilateral cleft lip which has normal Cupid’s bow in one side and abnormal one in cleft side, the flap can be transferred from contralateral side to restore volume and symmetry in upper lip.
The lower lip asymmetry is not as much noticeable as in upper lip, if it is not over 7 mm wide of flap size in unilateral cleft lip deformity. The flap width should not exceed 10 mm wide to prevent eminent deformity and unnatural movability of lower lip so far as in bilateral cleft lip deformity. Although some studies suggest 10 to 15-mm width for optimal flap size, the characteristics of the upper and lower lips of each patient were taken into account to determine the appropriate size [10]. The lengths of the upper and lower lips in each patient were measured before entering and in the operating room, and the flap size was decided based on the subtracted value of the two lengths.
Pedicle was divided 9 days after the surgery in the unilateral cleft lip patients, and 10 days in the bilateral cleft lip patients. A report suggest even waiting only 5 days before severing the pedicle is safe enough [11]. However, there was concern of patients’ movement of the attached lips, compromising the vascular supply, since the patients were discharged after the initial surgery. Furthermore, the pedicle was not divided before testing of the flap viability via ligation. Cleft lip patients usually require further scar revisions of the resulting upper lip scar from previous surgeries, and upper lip scars resulting from Abbé flap can be corrected simultaneously. Thus, the scar from delaying flap division and insetting was not such a big concern. The safety of the flap was on the highest priority.
One usual complaint of patients with Abbé flap is new and additional scar on upper and lower lip. In conventional technique or other modifications, long scar of lower lip and multiple linear scars on upper lip were inevitable. In this technique, lower lip scar is limited to labiomental sulcus and shaded area which scar can hide even in frontal view. In terms of upper lip, no new scar is formed on philtral area except small transverse short scar whose height is less than 2 mm. Furthermore, in unilateral cleft lip patients, no scar is formed even in the upper lip mucosa by using existing scar from primary repair. This is the major advantage from other techniques, which leave long and highly-visible scar on upper and lower lip, occasionally extending to nostril sill. Minimal intervention induced the best result on esthetic and functional aspect on both upper and lower lip.
Small amount of tissue dissection and flap harvesting contribute to excellent versatility of the flap. No complication was shown regarding flap loss or even marginal necrosis. The flap color and volume showed disharmonious with adjacent vermilion mucosa which was turned into similarity over time. Some patients had notching of insertion site on mucosa, which were resolved with simple scar revision.
One additional benefit of this technique is improved of upper and lower lip relationship in lateral profile. Almost secondary cleft lip patients usually have unfavorable profile resulting from retrusion of upper lip and greater volume and eversion of lower lip especially in mandibular prognathism. This makes the lower lip protrusion and ectropion with opening mouth. This technique makes the lower lip tightening and closing mouth with more harmonious profile on lateral view (Figs. 2E, F, 3C, D, and 4C, D).
In conclusion, secondary cleft lip patients suffer from shortage of upper lip tissue, and Abbé flap can be effectively applied in these patients. A novel modification of Abbé flap can be one of the substitutes for correction for lack of central lip tubercle and deformities of Cupid’s bow. Outcomes were promising, especially in aesthetic point of view.
Notes
No potential conflict of interest relevant to this article was reported.
Notes
PATIENT CONSENT
The patients provided written informed consent for the publication and the use of their images.