Columellar reconstruction: a refinement of technique
Article information
Abstract
The nose is an important landmark of the face and its shape and beauty is of significant concern. The columella is the subunit between the two nostrils that provides support and projection to the nasal tip and has functional role in nostrils, as well as aesthetic. Ethiology for columellar absence or deficiency is diverse, and it is one of the most complex nasal subunits to reconstruct because of its narrow horizontal dimension, its tenuous vascularity and limited availability of adjacent tissue. We present a patient with columellar, membranous septum and upper lip defect, due to oncological resection. The lip reconstruction was designed using advancement of two upper lip edges with the technique of webster perialar/nasocheek advancement. However, the perialar/nasocheek tissue which is usually discarded was used as inferiorly based skin flaps to reconstruct the membranous septum, columellar skin and nasal vestibule lining. Rib cage cartilage graft was used as columellar strut for support. At 1-year follow-up, the patient has good nasal contour and projection. Scaring of the columella is very subtle. This is a versatile way for successful reconstruction of a columella and large central facial defect in one-stage operation. It is a method which provides very satisfactory aesthetic result with minimum patient morbidity and discomfort.
INTRODUCTION
The nose is an important landmark of the face and its shape and beauty is of significant concern since ancient times. The columella is the subunit between the two nostrils that, along with the lower lateral cartilages and caudal septum, provides support and projection to the nasal tip. It plays a functional role in nostrils patency and nasal breathing [1], and also of major aesthetic significance. Columellar absence or deficiency may occur as a result of tumor resection, bilateral cleft lip, trauma, or cocaine abuse [2-4]. The columella has repeatedly proven to be one of the most complex nasal subunits to reconstruct because of its narrow horizontal dimension, unique contour, its tenuous vascularity and limited availability of adjacent tissue [2]. The need for a reconstruction that will provide the necessary structural and aesthetical properties of the columella, often necessitates multiple stages. The goal of this paper is to report a case of successful complex one stage columellar reconstruction after oncological resection and to discuss the technique and possible alternatives.
CASE REPORT
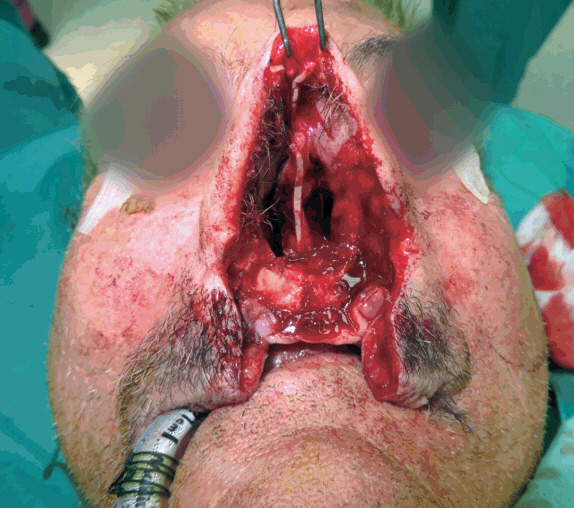
A 75-year-old male patient underwent excision squamous cell carcinoma, arising from his columella (Fig. 1). The resection resulted in a defect involving the whole columella, membranous septum, bilateral aspect of nasal sill, and the medial aspect of upper lip that constituted about 25% of the upper lip width (Fig. 2). The lip reconstruction was designed using advancement of two upper lip edges with the technique of webster perialar/nasocheek advancement. However, the perialar/nasocheek tissue which is usually discarded was used as inferiorly based skin flaps in a sail shape to reconstruct the membranous septum, columellar skin and nasal vestibule lining (Figs. 3, 4).

Squamous cell carcinoma of columella.
Defect of columellar, membranous septum and upper lip.
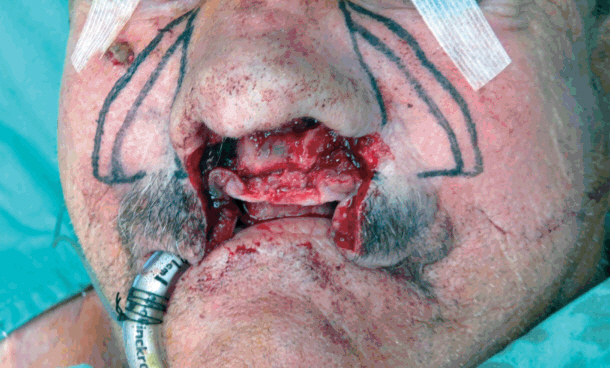
Planning of inferiorly based sail-shaped flaps.

Sail-shaped flaps brought to reconstruct nasal septum and columella.
The most lateral aspect of the sail-shaped flap was sutured to the most inner part of the defect at the nasal floor and septum junction thus creating a pocket. Rib cage cartilage graft was used as columellar strut for support. The cartilage was fixed to the septum remnant with 5-0 PDS suture. The two medial aspects of the nasolabial flaps were sutured together in the midline. Donor site in the nasocheek areas were closed primarily with no remarkable disfigurement (Figs. 5, 6). Postoperative period was uneventful. At 1-year follow-up, the patient has good nasal contour and projection. Scaring of the columella is almost undetectable (Figs. 7, 8).

Postoperative basal view.
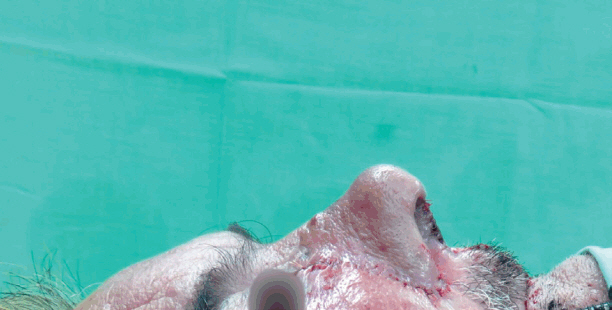
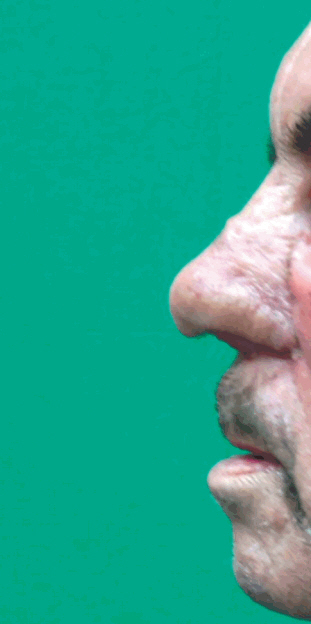
Postoperative lateral view.
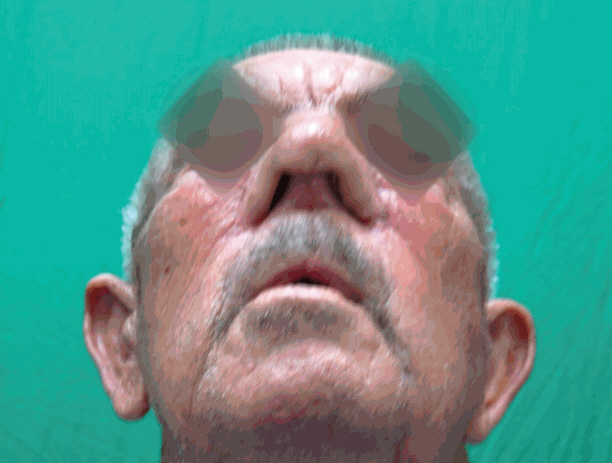
One-year postoperative basal view.
One-year postoperative lateral view.
DISCUSSION
Columellar defect or absence may be a result of variety of pathologies. Reconstruction of this delicate central subunit is difficult and challenging because of its narrow horizontal dimension, unique contour, its tenuous vascularity and limited availability of adjacent tissue [2]. Few methods were proposed for this purpose: use of composite grafts [5,6], nasolabial flaps [7,8], nasocheek flaps [9,10], buccal mucosal flap [11], free flap [2], forehead flap [12] and prefabricated flaps [13]. We used nasocheek flaps reconstruction which is a modification of a method described by Akbas et al. [10], which failed to provide sufficient nasal tip support as they discussed. The use of septal cartilage for support as previously described by Jayarajan [9] may not always be available due to the posterior extant of the defect as well as in cases of previous septal surgery or nasal trauma. Some have proposed the use of ear cartilage which is also limited in its amount and strength. The usage of costal cartilage has the advantage of virtually “unlimited” amount as far as nasal reconstruction and is the mechanically stronger. The cones of costal cartilage are donor site scar and higher degree of surgical skills needed for safe harvest.
We described a safe and versatile way for successful reconstruction of a columella and large central facial defect in one-stage operation. It is a method which provides very satisfactory aesthetic result with minimum patient morbidity and discomfort.
Notes
No potential conflict of interest relevant to this article was reported.
Notes
PATIENT CONSENT
The patients provided written informed consent for the publication and the use of their images.