INTRODUCTION
Calcinosis cutis is a rare disease consisting of deposition of calcium salts in the skin and subcutaneous tissue and can be classified as dystrophic, metastatic, idiopathic, or iatrogenic [1,2]. Tumoral calcinosis is a special form of the idiopathic calcinosis cutis and was first named in 1943 by Inclan et al. [3,4]. Tumoral calcinosis presents as a painless, firm, tumor-like mass and is commonly found around the hip, shoulder, elbow, and knee joints [3]. However, tumoral calcinosis of the auricle is extremely rare. We present the case of a 13-year-old boy with tumoral calcinosis of the helix of the ear auricle.
CASE REPORT
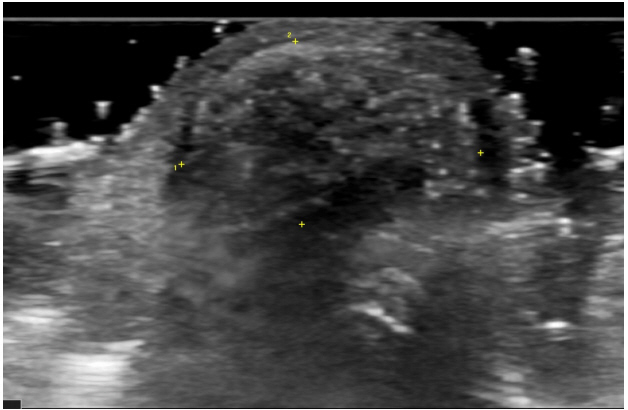
A 13-year-old boy presented with a chief complaint of a growing mass on the helix of left auricle for 10 years (Fig. 1). It was hard and painless, with non-tender and non-compressible swelling. There was no history of trauma on the auricle or any family history of tumor disease, except for presence of keloid skin in the mother. Ultrasonography investigation revealed a 1.15├Ś0.7├Ś1.45-cm heterogeneous hyperechoic mass on the helix of the left auricle (Fig. 2), which was clinically diagnosed as cartilage-origin benign neoplasm.
Under local anesthesia, complete surgical excision of the tumor was performed. A vertical incision was made through superior helix. The tumor was removed entirely by delicate dissection. The tumor appeared to be well circumscribed, hard, spherical mass measuring about 2 cm in diameter (Fig. 3).
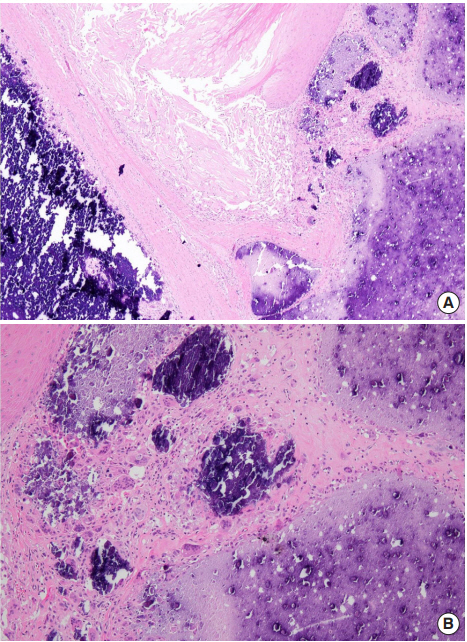
The histopathological examination result showed that normal auricle structure was hardly visible, and extensive calcification was seen as a purple-blue, homogenous material. Dense hyalinized stroma surrounded the calcified material with formation of multiple cystic spaces and progressive calcification with eosinophilic debris (Fig. 4A). Foreign body giant cell reaction with calcification and epithelioid cell were also observed (Fig. 4B).
A diagnosis of tumoral calcinosis was confirmed. The patient was discharged following surgery, with no complaint of discomfort. The patientŌĆÖs lab values were serum phosphorus 4.7 mg/dL and serum calcium 9.4 mg/dL, all within normal limits. After 9 months of follow-up, there were no signs of recurrence of the tumor (Fig. 5) and the patient was highly satisfied with the surgical results. We obtained the patientŌĆÖs medical records and reviewed the related literature. This study was approved by the Chonnam National University Hospital Institutional Review Board (IRB No. CNUH-2018-209).
DISCUSSION
Tumoral calcinosis is classified into three subtypes: primary normophosphatemic tumoral calcinosis, primary hyperphosphatemic tumoral calcinosis, and secondary tumoral calcinois. The first subtype often shows familial tendency and is most commonly seen in African patients. It also occurs sporadically and is associated with past trauma. The second subtype is a rare autosomal recessive disorder caused by mutation of the GALTN3 gene. The third subtype presents calcium deposits at multiple sites due to renal failure or renal dialysis. Normophosphatemic tumoral calcinosis has a better prognosis than other subtypes. Additionally, as each subtype has a different response to treatment, it is advisable to identify the subtype correctly [3,5-7].
In case of suspected tumoral calcinosis, plain radiographs can be taken to confirm amorphous calcification. Investigations like ultrasonography, computed tomography, etc., can aid in identifying the correct size and surgical planning. Magnetic resonance imaging scans show inhomogeneous, high-signal intensity on T2-weighted images and homogeneous, low-signal intensity on T1-weighted images [3,5,8]. Furthermore, serum calcium levels, serum phosphorus levels, serum parathormone levels, 1,25-dihydroxy-vitamin D levels, and renal function tests should be checked to classify the disease.
Other benign non-epithelial tumors of the ear auricle include cyst, keloid, hemangioma, hematoma, osteoma, and soft tissue chondroma, while malignant nonepithelial tumors include chondrosarcoma [9-11]. Therefore, a definitive diagnosis is needed and histological examination becomes essential. Histopathological examination of this case shows extensive calcification with surrounding dense hyalinized stroma. Foreign body giant cell reaction is also observed and epithelioid cells are seen in many cases [3]. Additionally, there was no history of trauma, specific reaction to foreign body, metabolic disorder, nor any significant family history, and the serum biochemical level was normal. Therefore, it was diagnosed as tumoral calcinosis, a subtype of idiopathic calcinosis.
The standard treatment modality for tumoral calcinosis is early surgical excision [3,5]. However, when there is a mass on the joint, recurrence rates tend to be higher in adults. Hence, in normo- or hyperphosphatemic cases, treatment with phosphate-binding chelating agents or acetazolamide may help to reduce recurrence rate of tumoral calcinosis. With accompanying renal failure, phosphorus restricted diet, dialysis, and phosphate-binding agents are the preferred treatment modalities [3]. On the other hand, surgical treatments such as parathyroidectomy or renal transplantation may be considered if the serum biochemical level is not under control.
Our study had the limitation that tumoral calcinosis of the auricle has not yet been established with respect to its nature, recurrence, and prognosis. Therefore, further studies and longterm data are required to establish biological understanding and treatment for patients. There are several possible tumors of the auricle, among which tumoral calcinosis is extremely rare and can be misdiagnosed as other tumors. Hence, accurate diagnosis is essential for therapy. Serum calcium, serum phosphorus, and gene analysis tests may also be performed when necessary. Surgical resection should be considered as the treatment of choice.