INTRODUCTION
Xanthelasma palpebrarum is the most common xanthoma occurring in the eyelids and the most common cutaneous xanthoma. It usually manifests as a flat, yellowish lesion that is clearly visible on the face, causing a cosmetic problem. Fatty deposits can produce a darker red or brown appearance, and variable texture and firmness [1]. The lesion can be soft, semisolid, or calcareous. It most commonly occurs near the inner canthus of the eyelid, more frequently on the upper lid [2]. This typically presents in middle-aged and elderly people, and more frequently in women [3]. Lesions progress slowly and do not regress without treatment. These lesions, although not potentially malignant, may lead to ptosis if they enlarge excessively [4]. Xanthelasma palpebrarum typically appears in the dermal layer of the face; consequently, cosmetic treatment is needed. However, in this report, we present a unique case of xanthelasma found only in the muscle.
CASE REPORT
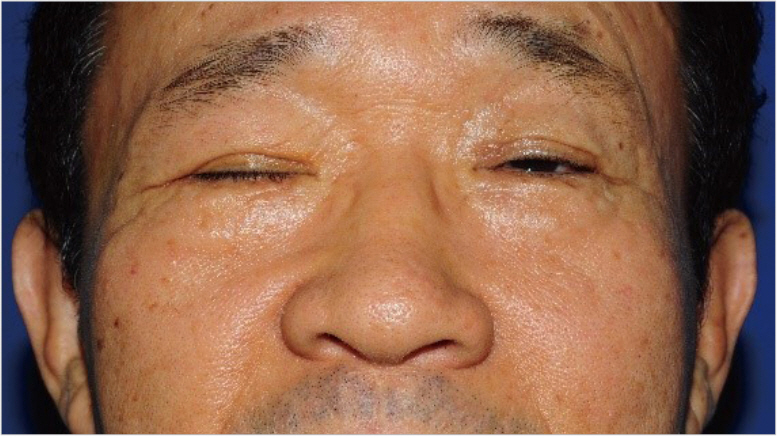
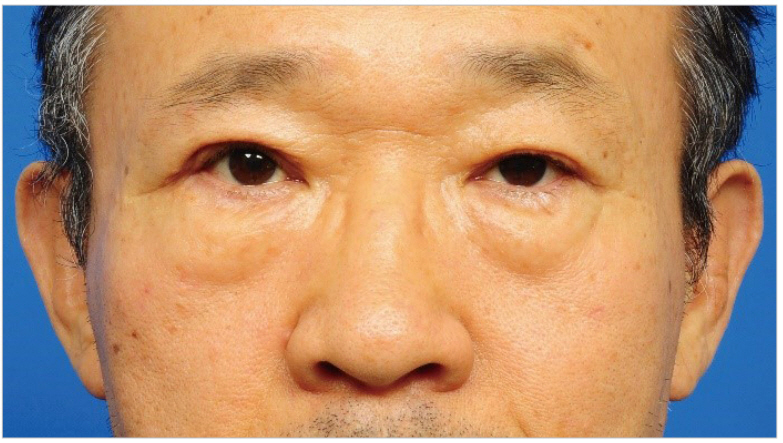
A 56-year-old man presented to our outpatient department with a chief complaint of right upper eyelid ptosis that appeared 2 months previously. He was feeling discomfort and heaviness while opening both eyes. He had bilateral blepharoptosis (more severe on the right side). Moreover, a small nodule could be felt under his right upper eyelid when touched, which was causing discomfort (Fig. 1). On physical examination, the nodule was very small, about 0.3Ć0.3-cm, and had the same skin color as the right upper eyelid. The patient did not feel any change in size over time, and no other lesions were found in his body.
He was admitted to our hospital because of sudden weakness on his right side 3 months previously, with a diagnosis of cerebral infarction of the basal ganglia. The blepharoptosis is presumed to be a secondary symptom due to his medical history. He had a history of vessel atherosclerosis and high-risk conditions including hypertension, diabetes, and dyslipidemia. Thereby, he was taking medications and his lipid profile was normal.
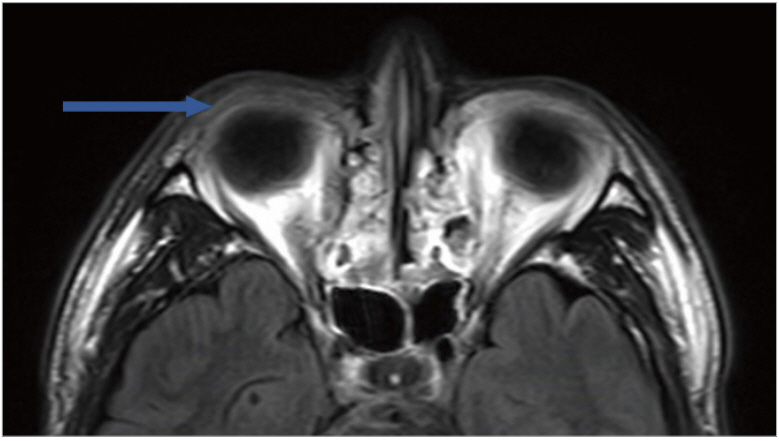
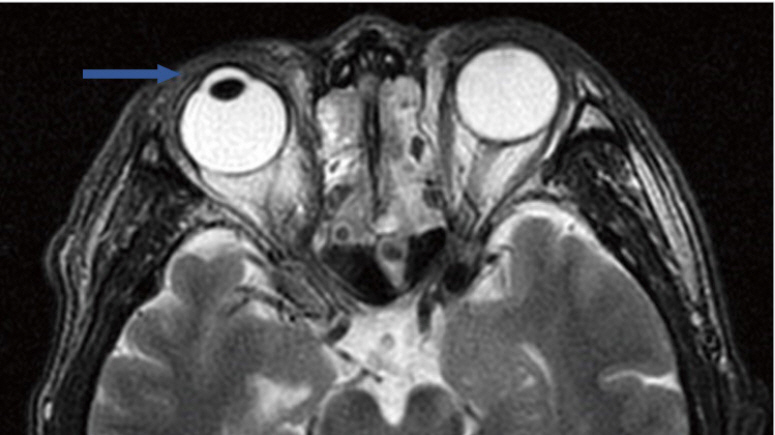
He underwent brain magnetic resonance imaging (MRI) to evaluate for cerebral infarction about 3 months before surgery. At this time, a white band, like adipose tissue, distinct from the orbicularis oculi muscle was observed in the right upper eyelid in the T2 image (Fig. 2). On brain MRI T2 images, this lesion disappeared after about 2 months (Fig. 3).
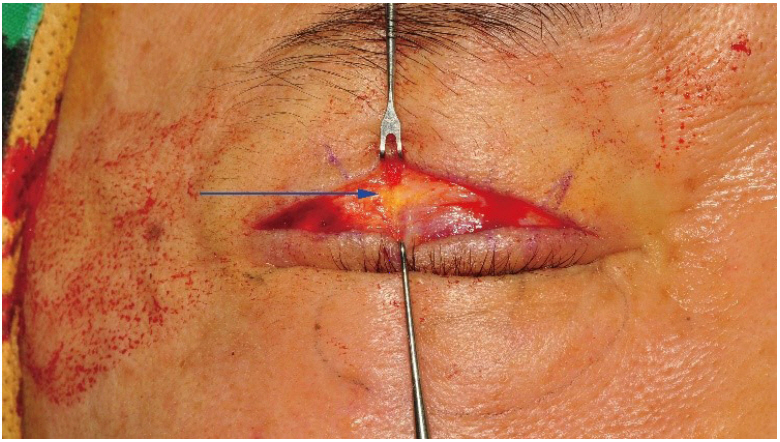
The surgery was designed with a blepharoplasty incision line to correct both blepharoptosis. To check for levator aponeurosis, the subcutaneous fat layer and orbicularis oculi muscle were dissected in the right upper eyelid. A yellowish lipid-like band different from normal tissue was found in the orbicularis oculi muscle (Fig. 4). A 0.3Ć0.3-cm round mass, which was suspected to be the cause of the patientās discomfort, was identified (Fig. 5). The band was excised with the nodule. After removal of the nodule, weakness of levator aponeurosis was confirmed and corrected by securing the fixation of levator aponeurosis to tarsal plate.
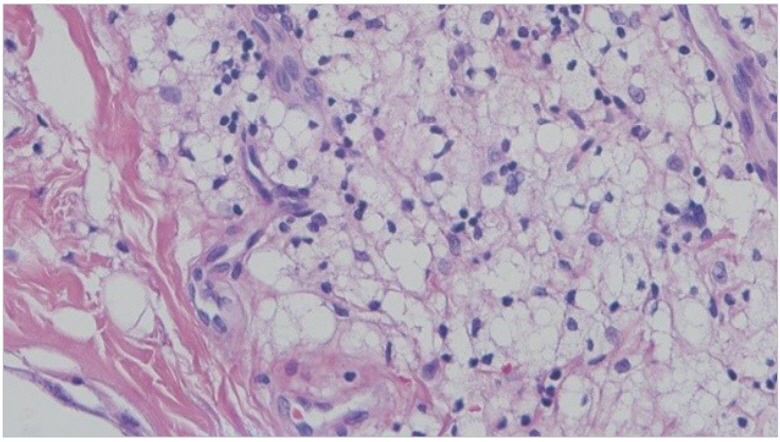
On histologic analysis, the excised mass consisted of lipid-laden histiocytes in the periphery of the blood vessels along with cluster of foamy cells, which was confirmed as xanthelasma (Fig. 6). The orbicularis oculi muscle and lacrimal gland around the lesion demonstrated chronic inflammation with foreign body reaction and tissue fibrosis. About 6 months after surgery, the foreign body sensation in the right upper eyelid disappeared and the patient was satisfied with the aesthetic outcome (Fig. 7).
DISCUSSION
Histologically, xanthelasma is similar to other xanthomas, which are associated with hypercholesterolemia and composed of foamy histiocytes with occasional Touton giant cells [5]. These tend to aggregate around blood vessels in the superficial dermis and periadnexal locations, and are accompanied by peripheral fibrosis and inflammation [1]. It has been suggested that trauma and inflammation may alter vascular permeability, allowing lipoproteins to enter the dermis and subsequently become phagocytosed by dermal cells [5]. Moreover, there is some similarity between xanthomas and atheromas, at least experimentally. Foamy histiocytes have a perivascular arrangement, which implies that their stored lipid originates from plasma lipids [5].
Abnormal lipid metabolism seems to be important in the pathogenesis of xanthelasma. Cholesterol entering xanthomas along the capillary walls is mostly low-density lipoprotein (LDL), suggesting that the accumulated cholesterol is derived from blood [6]. Consequently, perivascular permeability increases and the blood vessel lipids are released and phagocytosed by dermal cells. These cells form the foamy histiocytes causing inflammation and fibrosis in surrounding normal tissues. When yellowish cholesterol-rich material in large foam cells accumulates in the skin and tendons, the clinical symptoms of xanthelasma become manifested [7].
Most cases of xanthelasma were diagnosed by clinical features. Most patients visit the hospital for cosmetic reasons, and they can be diagnosed visually by typical lesions. It can be confirmed by biopsy, but it is usually confirmed during surgical excision.
Treatment depends on the size and lipid profile. If there is abnormality in lipid profile, lifestyle modification or medication is recommended first. However, in cases of normolipidemic patients or those whose drug therapy is not effective, removal is performed by laser therapy, radiofrequency, cryosurgery, or trichloracetic acid when the size is small, whereas surgical excision is performed when the size is large [2]. But, in most cases the drug therapies are not effective, and most of them are removed through physical and chemical methods.
The causes of intramuscular xanthelasma in our patient can be divided into two main mechanisms. The first is related to systematic risk factors. Xanthelasma is known to be associated with atherosclerosis or dyslipidemia. The facts that many patients have associated disorders of lipid metabolism and that xanthoma cells frequently accumulate around blood vessels imply that the accumulated dermal lipid derives from the serum. According to previous studies, the incidence of atherosclerosis seems to be low in normolipidemic xanthoma and necrobiotic xanthogranuloma, whereas it is high in hyperlipidemic xanthoma [7]. Moreover, cholesterol storage in xanthelasma and atheroma plaque formation in vessels are experimentally similar [8]. In our case, the patient was taking hyperlipidemia medication, and he was receiving steady treatment for cerebral infarction 2 months previously. Therefore, he had more systematic risk factors that can generate xanthelasma than other people. Furthermore, hypercholesterolemic xanthomas also tend to result in a more nodular and tendinous type [5]. This may provide evidence for the higher possibility of onset of atypical xanthoma in these patients.
Second, in terms of local factors, the dermis of the eyelid is thin, and pulsatile pressure increases dermal capillary pressure during nictitation, which may occur 10ā30 times/min; this probably plays a role in lipid deposition in the eyelid [9]. These local factors could lead to the development of a lesion on the eyelids. However, why this condition develops only in the eyelids, and not in other sites, as a leakage phenomenon from capillaries, remains obscure. Several suggestions can be made about this issue. This area has exceedingly rich vasculature. Fluid may accumulate early in the dermis of the eyelids in systemic diseases such as nephrotic syndrome and congestive heart failure [10]. Another possibility is that many physical movements, such as blinking, increase local heat, which then increases the leakage rate. It has been shown experimentally that the rate of capillary leakage of LDL is twice as much in xanthomas that have been exposed to physical movements and friction than in xanthomas on immobilized cutaneous sites [5]. The eyelids are exposed to constant movement and friction, and this might be the reason why xanthelasma develops in these areas. These patients might also have intrinsic susceptibility to this capillary leakage [5].
Xanthelasmas are not limited to the superior dermis; they may penetrate the entire dermis and reach the orbicularis muscle. Mittelviefhaus et al. [11] suggested that xanthelasma can be divided into three categories according to depth, invasion into the dermis, and invasion adjacent to and into the stratum. Moreover, 42% of xanthelasmas infiltrate the entire dermis and reach the stratum or even invade into this layer [11].
Finally, from the histocytologic aspect, phagocytosis by dermal macrophages is important in the dermal layer of foamy cells found in xanthelasma, as mentioned above. The source of macrophages and histiocytes that cause this reaction is not only the dermis but also virtually all tissues. These cells are commonly found in all tissues where inflammatory reactions occur.
Thus, the theoretical background in which intramuscular xanthelasma can exist is sufficient, and cases infiltrated into the muscle have been reported. However, there have been no cases of xanthelasma within the only muscle.
Most patients with xanthelasma visit the hospital for the chemical or physical removal of cosmetic problems. However, physicians tend to focus on exposed skin lesions. As previously reported, xanthelasma may not be limited to the dermis; they may occur even in muscle. It may also be present only in the muscle. Therefore, imaging, histopathologic evaluation, and a cautious clinical approach are needed for patients with xanthelasma, and a multidimensional approach according to the depth of the lesion is needed for treatment.