INTRODUCTION
The nose is located in the center of the face, and the incidence of nasal bone fractures is on the rise [1-4]. Isolated nasal bone fractures usually require closed reduction procedures, and nasal bone fracture patients often have great interest in the appearances of their noses following the operation. After surgery, these patients examine their noses carefully to determine whether their nasal shapes have been changed.
In the past, many studies have measured the nose of healthy Korean subjects [5-8]. However, few studies have examined the nasal anthropometry of subjects who have experienced nasal bone fractures. This study aimed to investigate and explain changes in nasal shapes before and after surgery through objective photogrammetric anthropometry measurements taken through the three-dimensional (3D) reformation of computed tomography (CT) images.
METHODS
Patient evaluation
A database of patients who experienced nasal bone fractures between January 2016 and June 2017 was reviewed, and 100 patients over 20 years old who had isolated nasal bone fracture and underwent closed reduction procedure were included in the study. Patients who had congenital facial anomalies or had undergone any previous nasal surgeries were excluded. Clinical evaluations collected data on patient age, sex, and objective changes to the nose (both preoperatively and postoperatively) as measured by the height of the nasal base, length of the long nostril axis, the nasal alar angle and the amount of nasal deviation.
Surgical technique and time of CT scans
Closed reduction procedures were performed on all subjects while under general anesthesia. Pre-existing septal fracture or deviation was reducted conservatively. Following the reduction, Vaseline gauze was packed into the dorsal nasal cavity and Merocel (Medtronic Xomed, Jacksonville, FL, USA) was placed in the nasal airway with an external nasal splint. Examinations of preoperative CT scan were taken in day of injury visiting emergency room, and closed reductions were done about a week after the injuries. Examinations of postoperative CT scans were taken approximately 6 hours after the operations with removal of Merocel and nasal packings [9].
Photogrammetric nasal anthropometry
Nasal anthropometry was examined using the ruler tool in Adobe Photoshop CS3 (Adobe Inc., San Jose, CA, USA) through the 3D reformation of soft tissue made from CT scans that were taken with non-enhanced facial bone CT images with 2 mm sections (Dual 128-channel CT SOMATOM Definition Flash; Siemens Industries, Munich, Germany).
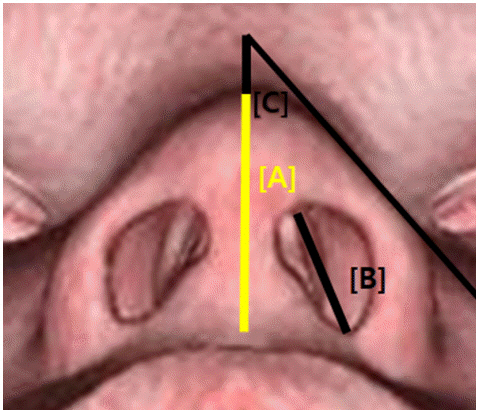
For objective measurements of nasal tip, the positions of the nasion and pronasale were adjusted to the same point in the basal view, and then, the height of the nasal base from the pronasale to subnasale, the nostril length of the long axis, and the nasal alar angles on both the right and left sides were also measured. Additionally, the changes between the right and left nostril lengths with the nasal alar angle were measured (Figs. 1, 2).
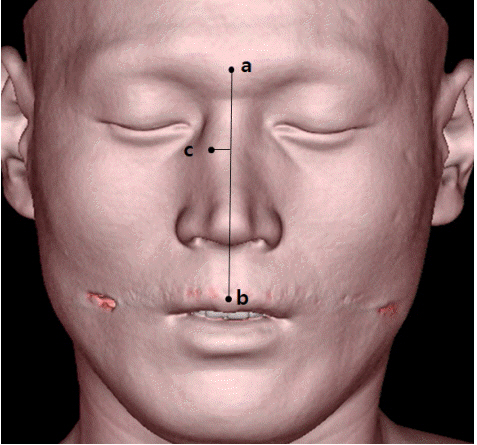
For measuring the nasal deviation, according to Frankfort horizontal line, amount of nasal deviation was measured on frontal view. We drew a vertical line from the midpoint of the glabella to the midpoint of the upper lip and marked the most prominent point of nasal dorsal deviation. Amount of nasal deviation was measured according to the length from the vertical midline to the point of most deviation on nasal dorsum (Fig. 3) [10].
RESULTS
Demographics
The 100 patients were all over 20 years old; 70 were male and 30 were female. The mean age was 41.08 years old.
Photogrammetric anthropometry of the nose
In terms of nasal base height, the mean preoperative value was 20.192 mm and the mean postoperative value was 21.384 mm (Table 1). The difference between the preoperative value and postoperative one was 1.192 mm (Table 1). The mean preoperative value for the length of the long axis of the right nostril was 11.929 mm, and its postoperative value was 12.629 mm; the mean preoperative value of the long axis of the left nostril was 12.262 mm, and its postoperative value was 12.952 mm (Table 1).
The difference in the diagonal length of nostril comparing both sides was 0.333 mm preoperatively and 0.323 mm postoperatively (Table 2). The mean value for the right nasal alar angle was 41.183° preoperatively and 40.338° postoperatively. For the left nasal alar angle, the mean preoperative value was 42.565° and the postoperative value was 41.381° (Table 1).
The mean deviation in the alar angle between both sides were found to be 1.382° preoperatively and 1.043° postoperatively (Table 3). The mean amount of nasal deviation were found to be 5.248 mm preoperatively and 1.024 mm postoperatively. The mean correction value of nasal deviation was found to be 4.224 mm (Table 4).
DISCUSSION
In cases of isolated nasal bone fractures, it is common to perform a closed reduction. Patients with nasal bone fractures are often curious about potential changes to their nasal shape following the operation. After experiencing a prominent nasal deformity caused by trauma, patients are usually highly concerned about returning to their prior nasal appearance after surgery. Although many studies have measured noses in healthy Korean subjects, few have compared changes between preoperative and postoperative nose shapes in patients with nasal bone fractures.
This study aimed to investigate and explain changes in nose before and after surgery of nasal bone fracture through nasal anthropometry. A direct anthropometry method is ideal, but this requires considerable time and repeated measurements. Therefore, many previous studies used indirect anthropometry methods, such as those using standardized clinical photography [11].
However, there may be intractable value discrepancies between direct and indirect anthropometry methods. Recently, it has been possible to take photogrammetric anthropometric measurements through 3D image from soft tissue reformation as result of the increased utilization and quality of CT scanning. Many studies have analyzed the accuracy of anthropometry based on CT imagery. Today, it is commonly agreed that indirect anthropometry through 3D reformation is no different than direct anthropometry [12,13]. Thus, we evaluated nasal shape through indirect anthropometry using a 3D reformed soft tissue image. As most patients are more interested in their external nasal appearance than in how their reduction was performed, this study used nasal photogrammetric anthropometric measurements to evaluate how much external nasal shapes change following nasal operations.
For the height of nasal base, a mean value change of 1.192 mm was observed (Table 1). The differences in diagonal nostril length between both sides were 0.333 mm preoperatively and 0.323 mm postoperatively. The changed amount after operation was 0.010 mm (Table 2). The deviations of both nasal alar angles were 1.382° preoperatively and 1.043° postoperatively. The correction amount was 0.339° (Table 3).
We also evaluated external nasal deviation by measuring amount of dorsal deviation and found how much nasal deviation was corrected after operation. The mean preoperative amount of nasal deviation was 5.248 mm, and the mean postoperative deviation was 1.024 mm. The mean correction value of nasal deviation was 4.224 mm.
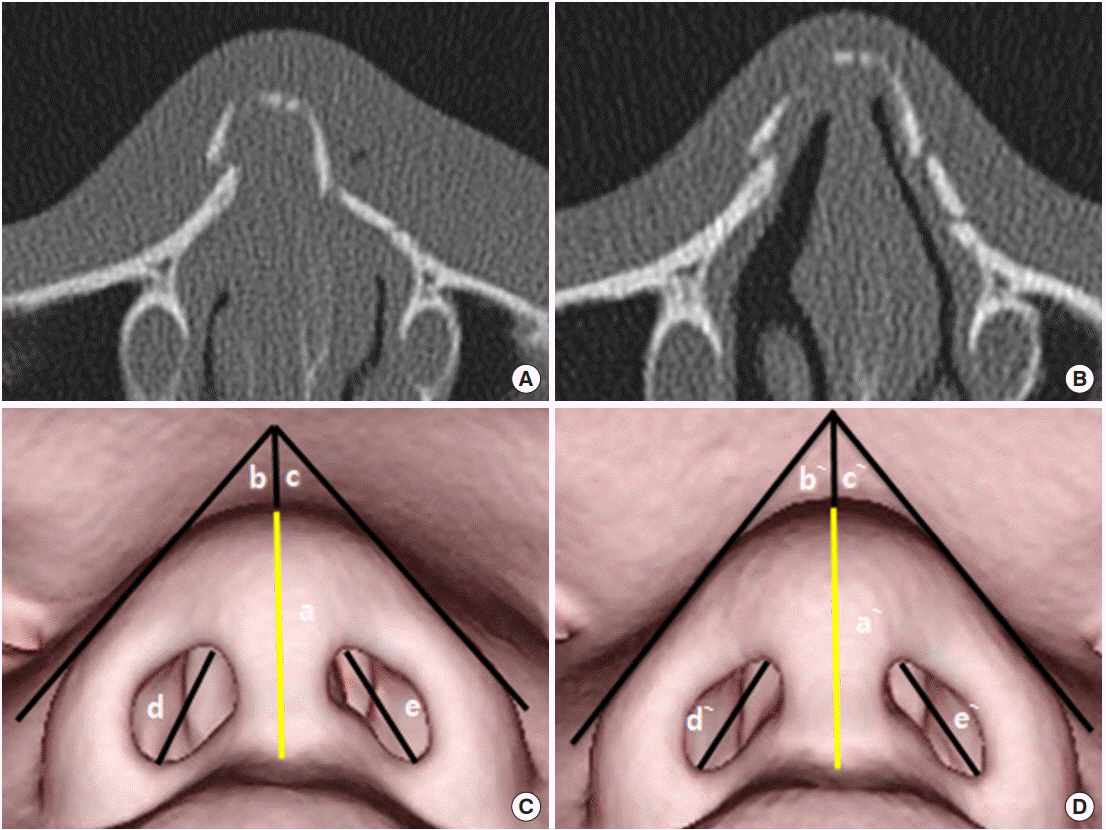
The residual deviation of the nasal dorsum after operation was not found to be significant, but acceptable. These results show that changes to nasal dimension after reduction operation were more noticeable in terms of nasal deviation and less noticeable in nasal tip, except for alterations in nasal alar angles between both sides (Figs. 4, 5). However, these results may be considered inaccurate due to nasal swelling discrepancies resulting from patient variations from the time of injury to the time of the operation.
Since the surgeries were performed approximately a week after trauma and the CT scans was examined on the day of surgery, it is thought that there were gaps of about a week between the preoperative and postoperative comparisons of CT images, resulting in a discrepancy in the state of nasal swelling between patients.
Even though the postoperative CT scans were examined the day of surgery, the nose tended to be less swollen after the procedure than in the preoperative state. Therefore, 3D reformations and objective measurements could be useful in evaluating both preoperative and postoperative nasal shape even before in period of stabilization after a sufficient period of time after surgery. Further, nasal shape improvements following nasal bone fracture surgeries were noted through changes in the nasal dorsal deviation and in the nasal alar angle between both sides.
In summary, it can be seen that after reduction procedures, changes in nasal dimensions were noticeable in terms of nasal deviation and less significant in nasal tip, except for changes in the nasal alar angle. This study may be useful when consulting with patients who have experienced nasal bone fractures and need surgical treatment.