Comparison of complete surgical excision and minimally invasive excision using CO2 laser for removal of epidermal cysts on the face
Article information

Abstract
Background
Epidermal cysts are benign, slow growing cysts that often develop on the head, neck, chest, and back of adults. The most common method of surgical excision involves the use of a scalpel and often leaves a scar proportional to the size of the cyst. Therefore, minimally invasive techniques are required. Among these techniques, the CO2 laser-based technique is minimally invasive and has lower complication rate, shorter recovery times, and lesser scarring. This paper aimed to compare the results and postoperative complications associated with a CO2 laser-based excision against conventional surgical excision for epidermal cysts.
Methods
We surveyed 120 patients, aged 16 to 65 years, with epidermal cysts on the face measuring 0.5 to 2.2 cm in diameter. Twelve months later, we compared the scar length, recurrence rate, patient satisfaction, and complications between patients treated with CO2 laser excision versus surgical excision.
Results
The mean scar length (12 months postoperative) after CO2 laser excision was 0.30± 0.15 cm, and that following surgical excision was 1.23± 0.43 cm (p= 0.001). The procedure time (time from incision after local anesthesia to the end of repair) was 16.15± 5.96 minutes for CO2 laser excision versus 22.38± 6.05 minutes for surgical excision (p= 0.001). The recurrence rates in the surgical excision group and CO2 laser excision group were 3.3% and 8.3%, respectively; this difference was not statistically significant (p= 0.648).
Conclusion
The cosmetic outcome of CO2 laser excision is excellent. For epidermal cysts measuring 2.2 cm or smaller, CO2 laser excision is recommended, especially when aesthetic outcome is considered important.
INTRODUCTION
Epidermal cysts are benign, slow growing cysts that often develop on the head, neck, chest, and back of adults. Surgical indications for epidermal cysts include pain or complications such as inflammation and infection; cosmetic effect is also an indication for resection [1]. The most common surgical technique is to make an incision using a scalpel on the skin, followed by complete surgical excision. This technique leaves a linear scar proportional to the size of the epidermal cyst [2-8].
Anatomically, the apex of an epidermal cyst is attached to the dermis of the skin. The remaining portion of the epidermal cyst is freely movable and loosely attached to the subcutaneous tissue. Recently, on this anatomical basis, various minimally invasive excision techniques have been introduced. Minimal invasive excision employed in previous studies, include laser punch, and biopsy punch incision. These methods are less invasive than complete surgical excisions; they do not require sutures and minimize scaring, and are thus considered more effective for an epidermal cyst on the face, where a scar is easily visible [3].
The author has been using a CO2 laser-based method as a minimally invasive excision [4]. As this method creates a small hole in the skin using a CO2 laser, complications such as hemorrhage or hematoma will be less common compared to techniques requiring an incision. In addition, recovery time is shorter, and the length of the scar, patient satisfaction is also expected to be shorter. This paper aims to compare the results and postoperative complications associated with the CO2 laserbased excision against conventional surgical excision for epidermal cysts.
METHODS
In Busan Paik Hospital, we surveyed 120 patients, aged 16 to 65 years, with epidermal cysts on the face measuring approximately 0.5–2.2 cm in diameter. This was a retrospective study in which the grouping method was limited to the patients’ faces, where the cysts were aesthetically visible. Size of the epidermal cyst was measured using ultrasound by a radiologist. In addition, complete excision and CO2 laser excision groups were randomly assigned. Exclusion criteria were 3 cm or larger cyst in size, recurring cysts, malignancy cysts, unconfirmed diagnosis, and cysts not on the face.
For treatment of the epidermal cysts, patients were divided into two groups: those treated with a CO2 laser (60 patients) (Fig. 1) and those treated with conventional surgical excision (60 patients) (Fig. 2). After an average follow-up of 12 months, the scar, recurrence rate, patient satisfaction, and complications were compared between the groups.

(A) A 36-year-old male with an epidermal cyst on the left cheek. (B) Patient’s photograph 12 months after CO2 laser excision.
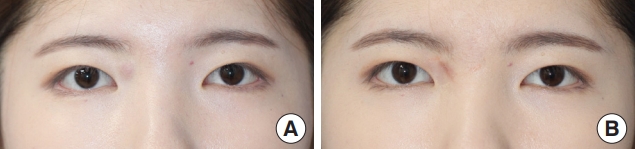
(A) A 20-year-old female with an epidermal cyst on the upper eyelid. (B) Patient’s photograph 12 months after surgical excision.
The surgical procedure was as follows. First, for the conventional surgical excision, the skin layer was incised elliptically or in a straight line to be removed under local anesthesia, and then exfoliation was carefully carried out using forceps so as not to break the cyst wall, followed by removal of the cyst wall. Next, the incised part was sutured. For the minimally invasive method, a hole of 2–3 mm was made at the pore in the upper part of the cyst using the CO2 laser. Most of the sebum in the cyst was extracted through the hole by gentle compression with gauze. One leg of a mosquito hemostat was inserted into the cyst, and the cyst wall was gently scraped away toward the hole using the horizontal grooves of the hemostat leg. Then, the skin wound was primarily sutured.
Patients were followed up with a 12-month postoperative office visit to measure the scar length and record complications. All patients were contacted by phone to inquire about recurrence of the cyst after 4 months and 12 months separately.
The Student t-test was used to evaluate normality of the data. SPSS software version 11.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analyses. p-values less than 0.05 were considered significant.
RESULTS
One hundred and twenty patients, aged 16 to 65 years with ruptured epidermal cysts on the face were included (Table 1). The mean preoperative cyst size for the surgical excision group was 1.31±0.55 cm, and that for the CO2 laser excision group was 1.20±0.37 cm (p=0.215) The mean scar length in the surgical excision group was 1.23±0.43 cm, and that after CO2 laser excision was 0.30±0.15 cm (p=0.001). The procedure time (time from incision after local anesthesia to the end of repair) was 16.15±5.96 minutes for the CO2 laser excision, much shorter than that of the surgical excision group (22.38±6.05 minutes, p=0.001) (Table 2).
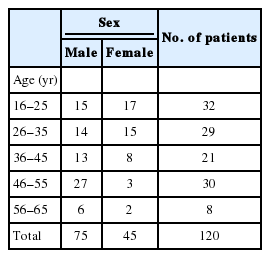
Patient demographics
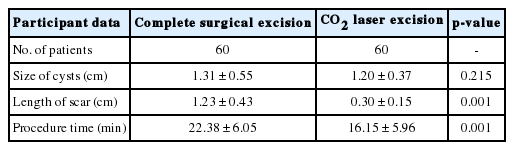
Clinical data for 120 patients with epidermal cysts
Concerning postoperative complications, wound dehiscence developed in two patients in the surgical excision group (3.3%); additional repair was performed for these patients. There were no cases of wound dehiscence in the CO2 laser excision group, but the difference between the two groups was not statistically significant (p=0.154). Postoperative hematoma was observed in three patients in the surgical excision group (5%) and no patients in the CO2 laser excision group; this difference was not statistically significant (p=0.079). The incidence of recurrence with both techniques is shown in Table 3. Early recurrence (0–4 months) rates in the surgical excision and CO2 laser excision groups were 0% and 3.3%, respectively; however, the difference was not statistically significant (p=0.672). Moreover, late recurrence (4–12 months) rates in the surgical excision and CO2 laser excision groups were 3.3% and 5.1%, respectively, but the difference was also not statistically significant (p=0.683). Similarly, the recurrence rates during the entire period (0–12 months) in the surgical excision and CO2 laser excision groups were 3.3% and 8.3%, respectively, but the difference was not statistically significant (p=0.648).

Postoperative complications
All 120 patients were contacted to inquire about their satisfaction with the scar; the results revealed that the CO2 laser excision group had a significantly higher satisfaction than the surgical excision group (Table 4). There was a statistically significant difference between the complete surgical excision and the CO2 laser excision group for the mean of the satisfaction scar scale. The difference was statistically significant (p<0.05) (Fig. 3).
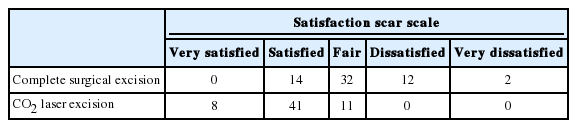
Results of satisfaction survey conducted 12 months after surgery
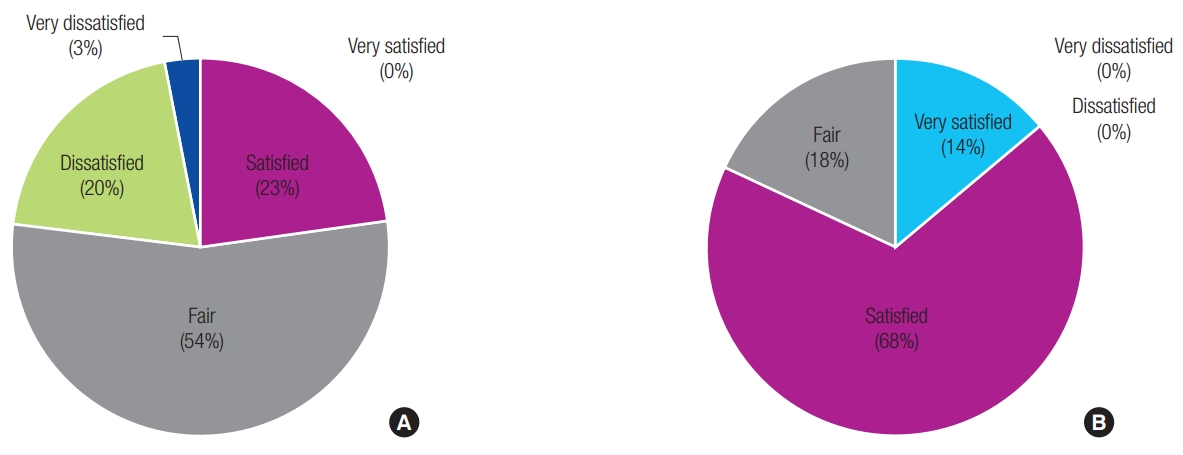
There was a statistically significant difference between the complete surgical excision and the CO2 laser excision group for the mean of the satisfaction scar scale. (A) Satisfaction survey result of complete surgical excision after 12 months. (B) Satisfaction survey result of CO2 laser excision after 12 months. Score of satisfaction scar scale: 5 (very satisfied), 4 (satisfied), 3 (fair), 2 (dissatisfied), 1 (very dissatisfied).
DISCUSSION
Recently, various new methods have been introduced to minimize scarring after surgical removal of epidermal cysts; these include delayed excision of the cystic wall after sebum evacuation by laser punch [3], cyst removal through a minimal incision [5], and cyst removal with a biopsy punch incision [6]. These methods have advantages of simplicity, reduced invasion, less bleeding, reduced scarring, and decreased healing time [8].
Among these minimally invasive techniques, we prefer using CO2 lasers in our hospital. The reasons are smallest incision size, no risk obstruction of the operative field by bleeding, and reduced risk of complications, such as hematoma. In addition, when perforating the cyst, creating a hole with CO2 laser allows the operation to be performed more neatly than making an incision with a blade.
The method using CO2 laser is a slightly modified version of using a stab incision. While the two methods share some similarities, they have distinct differences. First, there is a difference in the incision size. Although the difference in size is small, using CO2 laser can reduce scarring, which represents a significant difference in aesthetically sensitive areas in the face.
Second, bleeding is unavoidable with a stab incision, which can obscure the field of view. Accordingly, a bigger incision may be required or it may become difficult to neatly remove the cyst. Using CO2 laser allows bleeding to be controlled simultaneously with the incision. This makes it possible to perform the surgery without obscuring the field of view and allows visual confirmation of the cyst wall, based on which, the cyst wall can be perforated accurately.
The current results show that the minimally invasive method using a CO2 laser reduced not only the size of the postoperative scar but also operative time; these differences were statistically significant. These results can be a basis to support the use a CO2 laser as a primary treatment for epidermal cysts on the face, where scars are easily visible. Even for ruptured epidermal cysts, surgery can be considered after creating a hole using a CO2 laser, extracting pus and then stabilizing the patient so as to reduce scars. CO2 laser excision, in comparison with other minimally invasive methods (punch biopsy), results in better hemostasis and reduced hematoma development [4].
Wound dehiscence and hematoma, which can occur after surgery for epidermal cyst, were not observed in the group treated with the CO2 laser excision. However, in comparison with the complete surgical excision group, the difference was statistically insignificant. For minimally invasive excision using a CO2 laser, a statistically significant difference might can be obtained if a greater number of cases were included, as the CO2 laser can reduce the length of incision and thus improve control of bleeding.
There was no statistically significant difference in the recurrence rate between the two groups. Complete excision can be more difficult with the minimally invasive method using a CO2 laser compared to surgical excision, and thus may lead to recurrence. In addition, CO2 laser excision can leave a residual cyst wall that can lead to higher frequency of recurrence than that with the complete excision method. In the present study, a patient suffered from recurrence after a month, which was a case of a ruptured cyst being excised by CO2 laser, making it difficult to remove completely. Hence, the recurrence appeared early after the procedure.
The present study was conducted for epidermal cysts that were 0.5–2.2 cm in size. If the cyst size is larger or smaller than this, it is expected that there would be smaller scars, regardless of the size, as per the results of the present study; furthermore, CO2 laser excision would result in higher patient satisfaction than surgical excision.
Notes
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Ethical approval
The study was approved by the Ethics Review Board of Inje University Health Center (IRB No. 19-0028) and performed in accordance with the principles of the Declaration of Helsinki. Written informed consents were obtained.
Patient consent
The patients provided written informed consent for the publication and the use of their images.