INTRODUCTION
Autologous fat injection (AFI) is performed widely in plastic surgery; it is used in cosmetic surgery for rejuvenation or volume augmentation of the face, breasts, and other parts of the body and in reconstructive surgery for the correction of contour deformities or the treatment of scar contracture or radiation injuries [1]. Autologous fat is considered to be an ideal filler material because it causes fewer adverse reactions than other fillers; furthermore, it is biocompatible because it is the patientâs own fat. Harvesting autologous fat using liposuction is a comfortable, repeatable, and low-cost procedure for most patients [2].
However, the main problem associated with AFI for augmentation is the variable rate of absorption or necrosis at the grafted site. Transplant survival rates measured in terms of absorption or necrosis range from 30% to 80% [3]. In light of this variation, surgeons often perform overcorrection or repeated procedures, but patients may experience discomfort and dissatisfaction, an increased financial burden from the expenses associated with these procedures, and morbidity or trauma at the donor site. The remaining fat after the injection is usually discarded, which has spurred surgeons to explore ways of utilizing that fat. Accordingly, it has become increasingly common to utilize fat that has been cryopreserved after the initial fresh fat graft [4]. However, the fat that is cryopreserved after grafting is retained as dead and fibrous tissue, which may be associated with an elevated risk of clinical complications, such as oil cysts [5-7].
Very few clinical studies have investigated complications related to the use of cryopreserved fat. In this study, we present an analysis of our clinical results from facial lipofilling, with a comparison between fresh fat and cryopreserved fat injections.
METHODS
We analyzed the clinical records of patients who underwent facial lipofilling within the past 10 years and collected information about the injection site, the amount of fat injected, the number of fat injections, side effects, complications, and management. Fat injection-related symptoms included infections or inflammatory signs such as swelling, a palpable mass, or tenderness on the face. We excluded patients with a history of skin care procedures, such as chemical peeling or laser treatment, and dermatological skin lesions, such as acne. Sixty patients received fat injections. Fifty-one of these patients had no abnormal symptoms, while the remaining nine had inflammation or infections. Fifty-three of the 60 patients received fat injections at our institution, including seven men and 46 women. Their mean age was 48.6 years (range, 21â77 years). Seven patients were excluded from the statistical analysis because they were referred to our institution with fat injection-related symptoms, but did not receive the injections at our institution.
The study was approved by the Institutional Review Board of Kyung Hee University Hospital (IRB No. 2019-09-042-003) and performed in accordance with the principles of the Declaration of Helsinki. Written informed consent was obtained from patients.
Surgical technique
Fat was processed by manual harvesting using a tumescent fluid technique from the thigh or lower abdomen and centrifuged at 3,000 rpm for 3 minutes aseptically. We did not use cell-assisted lipo-transfer. Fat injections were performed using blunt Coleman infiltration cannulas (styles I and II) with the retrograde linear thread and fan technique. We ensured that the injected fat was spread evenly, without accumulating at a single point. After the injection, we applied an open dressing without compression and prescribed oral antibiotics and anti-inflammatory medicines for 5 days and oral prostaglandin for 14 days. For subsequent injections, we used cryopreserved fat, which was prepared by thawing. Except for the thawing step, the procedure for injecting cryopreserved fat was the same as the usual method. We used the cryopreserved fat within 6 months of frozen storage.
RESULTS
Twenty-two patients had a single fresh fat injection, four patients had two or more fresh fat injections, 16 patients had one fresh fat injection and one cryopreserved fat injection, six patients had one fresh fat injection and two cryopreserved fat injections, and five patients had two fresh fat injections and one or more cryopreserved fat injections (Table 1, Fig. 1).
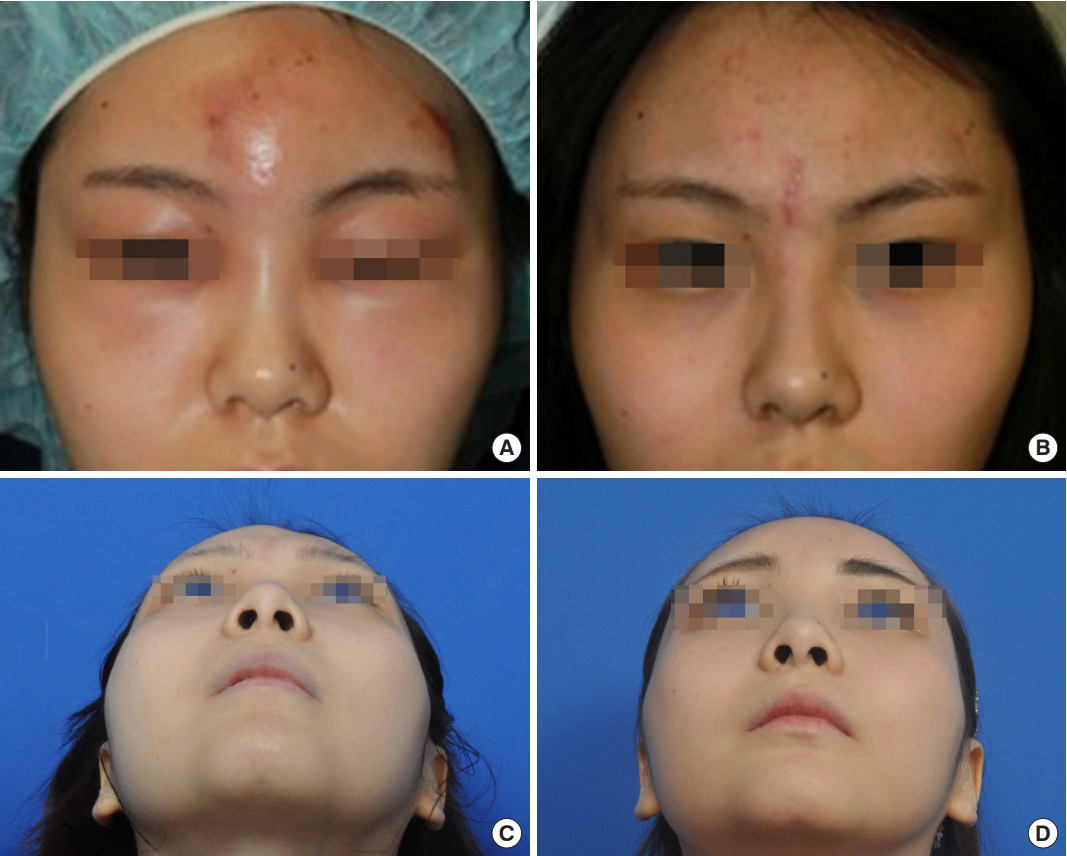
Overall, the most frequent site of fat injection was the nasolabial groove, followed in order by the cheek, forehead, and temples. However, the forehead was the most common site of injection in patients who received injections at only a single site. In total, 281 fat injections were performed, consisting of 170 fresh fat injections, 89 cryopreserved fat injections as the second injection, and 22 cryopreserved fat injections as the third injection. Complications occurred only in one patient, in whom signs of inflammation appeared after the second injection in the cheek, in which cryopreserved fat was injected (Table 2). The amount of fat injected by site and according to whether fresh or cryopreserved fat was used is shown in Table 3. The complication rate was 0.36% in all fat injections, 0.12% in second injections with cryopreserved fat, 0.90% in all cryopreserved fat injections, 3.57% in cryopreserved fat injections in the cheek, and 1.80% in fat injections. The mean interval between injections was 3.42 months (range, 1â8 months; data not shown). No complications occurred after fresh fat injections (the first injections). No statistically significant difference in the complication rate was found between patients who received only a fresh fat injection and those who received one fresh fat injection and one cryopreserved fat injection (p= 0.197). In the cheek, the complication rate was 1.47% of all fat injections, 4.76% of second injections, and 3.57% of cryopreserved fat injections. We found no statistically significant difference in the complication rate (p= 0.215) between patients who received one fresh fat injection and those who received second and third cryopreserved fat injections. Nine patients had inflammatory signs, of whom eight underwent surgical treatment, such as incision and drainage, curettage, and excision (Fig. 2). Of those patients, seven received a second injection containing cryopreserved fat, for a total of two injections at a 1- to 3-month interval, whereas the remaining patients received a cryopreserved fat injection at approximately a 1-month interval. The mean interval between the injections was 1.56 months.
DISCUSSION
In recent years, AFI has been performed widely in plastic surgery. Autologous fat is considered to be an ideal filler material because it causes fewer adverse reactions than other fillers; furthermore, since it is the patientâs own fat, it is biocompatible. Harvesting autologous fat through liposuction is a comfortable, repeatable, and low-cost procedure for most patients [2]. The American Society of Plastic Surgeons organized a task force to assess the safety and efficacy of autologous fat grafting and reported it to be safe and to have a low risk of complications [8]. Common complications of AFI include patient dissatisfaction, acne, calcification, infection, skin necrosis, hematoma, paresthesia, and asymmetric or irregular contours. Blindness due to occlusion of the ophthalmic artery and cerebral infarction are serious complications that have been reported in some cases. However, the main obstacle associated with AFI for augmentation is the unpredictability of the outcomes due to variable, but high, absorption or necrosis rates at the grafted site [3]. Due to the difficulty of predicting the final outcome, surgeons often perform overcorrection or repeated procedures, which may cause patients to experience discomfort and dissatisfaction, an increased financial burden from medical expenses, and morbidity or trauma at the donor site. For these reasons, multiple uses of cryopreserved fat may elevate the possibility of recipient-site complications, such as low-grade inflammation, fat necrosis, and infection.
The risk of contamination is higher for cryopreserved fat than for fresh fat. Fresh fat can be contaminated during basic processes such as harvesting and centrifugation, but cryopreserved fat can also be exposed to contamination during additional processing steps such as freezing, storage, and thawing. Microorganisms can grow at low temperatures and in anaerobic environments during storage, causing infections at the grafted site after a fat injection; such infections are problematic, even if the causative microorganisms are of low virulence [9]. Furthermore, free oil can form and cryopreserved fat can leak as a result of intracellular ice formation. In 1972, Mazur et al. [10] reported that below the freezing point, pure crystalline watercontaining ice grows and the unfrozen fraction in the space between the growing ice contains all cells and solutes. As cooling continues, the volume of the unfrozen fraction decreases and its concentration increases. The increased osmotic pressure causes water to flow out of the cells. However, an appropriately slow cooling rate ensures sufficient water efflux from the intracellular environment, minimizing intracellular ice formation. Ultimately, the viscosity of the unfrozen fraction becomes too high for any crystals to form, and the unfrozen fraction turns into an amorphous state without ice crystals. However, a very slow cooling rate can cause total dehydration, which is lethal to the cells. In contrast, when the cooling rate is too fast, there is inadequate time for water to leave the cells and intracellular ice forms, which results in cell death in the cryopreserved fat [10].
Controversy persists regarding the viability and safety of cryopreserved fat. However, the use of appropriate medical protocols and cryopreservation techniques can ensure higher levels of viability and safety, with lower risks of complications than other surgical procedures [11-13]. Freezing, storage, and thawing are also essential processes when using cryopreserved fat. Many studies have been conducted to determine the best freezing, storage, and thawing conditions for appropriate medical protocols and cryopreservation techniques. As mentioned earlier, in the freezing process, an appropriate cooling rate is required to prevent intracellular ice formation, with a widely used rate being 1°C/min. Cells frozen at â20°C were found to be more viable than those frozen at â196°C [14]. Furthermore, the longer the storage period, the less viable cryopreserved fat is obtained after thawing [15]. In the thawing process, the recovery rate of antioxidant capacity and the neutralization of oxygen radicals may increase with the thawing temperature. Hwang et al. [16] reported that rapid thawing of cryopreserved fat in a water bath at 37°C maintained high mitochondrial activity and minimized cell damage.
Staphylococcus aureus is a common cause of inflammation in patients who undergo cosmetic skin surgery. However, in cases of chronically persistent lesions that are slowly reactive or nonreactive to conventional antibiotics, the presence of nontuberculous mycobacteria (NTM) must be considered. In addition, if inflammation does not occur immediately after fat injection, it is necessary to consider the possibility of infection with atypical mycobacteria such as Mycobacterium chelonae and M. abscessus, known as rapidly growing mycobacteria (RGM) [17]. These cause skin infections through skin wounds from invasive procedures such as injection, tattooing, and liposuction [18]. Nonspecific symptoms, including painful nodules, swelling, and abscess formation, appear in patients with RGM infections [19]. In addition to the difficulties posed by their nonspecific presentation, atypical mycobacterium infections are difficult to diagnose using conventional methods. Acid-fast bacilli staining has been reported to be positive for only 11%â27% of cases in a previous study [20]. Compared with other methods, molecular biology techniques such as polymerase chain reaction (PCR) may be useful because of their high sensitivity and accuracy [21]. NTM infection may be considered if a delayed infection occurs after an AFI and conventional antibiotics are ineffective. Antibiotic sensitivity tests using empirical antibiotics and diagnostic methods such as PCR should be performed to diagnose an NTM infection [22]. If the treatment response is slow or no improvement is observed, surgical procedures such as debridement and excision might also be useful [23].
In the present cases, patients with signs of an acute infection were treated surgically. They experienced no recurrence and received an additional autologous fat graft for contour recovery. Surgeons who perform fat injections must keep in mind that lesions showing inflammatory signs after a fat injection will have a complicated clinical course. Moreover, although it was difficult to compare the referred cases and our cases, a marked difference was found between these groups in the interval between injections (1.56 months vs. 3.53 months). The survival rate generally stabilizes 3 months after the graft [24-28]. Furthermore, a longer interval is suitable for promoting the survival of previously inserted fat and recovery from the inflammatory environment induced by the fat injection. In addition, a large graft volume in a small area will show a lower survival rate compared than a small amount grafted in a large recipient area [29]. It has been reported that in Asians, a relatively large amount of fat must be injected into the forehead to create a thick blanket of fat for esthetic purposes, and under such circumstances, the anoxic central core of the grafted fat might be larger. The cheek looks like a basin and has a retaining ligament, the zygomaticocutaneous ligament (also known as McGregorâs patch) [30]. The small spot at the center of the depressed area requires much more fat to be grafted than the peripheral area, while the retaining ligament grabs the skin, preventing outward expansion. These factors may cause surgeons to overlook the effect of a graft or the presence of a new dimple, resulting in a tendency to perform overinjections, which carries the risk of complications. In any case, critical factors in micro-fat grafting include the relocation of mature adipocytes to the perfusion-rich layer and reduction of the anoxic central core fragment, resulting in failure of the apoptotic pathway [31]. We found no significant differences in the complication rate according to whether fresh or cryopreserved fat was used for AFI, indicating that careful handling and adequate technique protect from the anticipated complications of fat injection using cryopreserved fat.
A limitation of our study is its relatively small sample size. Moreover, it is necessary to study the relationships between complications and the interval of fat injections in patients who received facial lipofilling with a fresh fat injection followed by a cryopreserved fat injection on an atypical schedule.
Regarding the technique, elimination of free fat oil and nonviable components through centrifugation or mesh techniques may be useful for decreasing resorption [32] and the incidence of foreign body reactions. Furthermore, a blunt cannula, not a sharp one, should be used. Pre-tunneling and fat injection should be carefully and gently performed to prevent vessel damage because performing these procedures without a suitably delicate technique can cause fat embolism, resulting in serious complications such as blindness and tissue necrosis [9].
All injectable fillers cause normal foreign body reactions, which may develop into a foreign body granuloma in some patients. Depending on the injectable filler material, the histological reaction and permanence differ. The following five types of fillers are distinguished: autologous fat, natural fillers such as collagen and hyaluronic acid, fluid fillers such as fluid silicone and acrylamides, particulate materials such as polymethylacrylate, and microspheres such as resorbable dextran and polymethylmethacrylate [33]. As the immune response to various filler materials differs, and it remains unknown whether they cause late inflammation or granuloma formation, patients should be informed about the benefits and risks of cryopreserved fat injections, even autologous fat grafts, when choosing the appropriate fat injection technique.
In summary, clinical reports on the results of cryopreserved fat injections are rare. Our findings reveal no significant differences in the clinical outcomes of fat injections according to the use of fresh fat or cryopreserved fat. Accordingly, cryopreserved fat is a useful and safe resource for multiple fat injections, with advantages including aseptic fat handling and the delicacy of the technique.