INTRODUCTION
Velopharyngeal dysfunction (VPD) can be treated through non-surgical and surgical modalities. Surgical options include superiorly-based pharyngeal flaps, palatal lengthening (double opposing Z-plasty; Furlow palatoplasty), and sphincter pharyngoplasty. The most commonly used surgical technique for treating VPD following cleft palate repair is a posterior pharyngeal flap. Superiorly-based flaps are more effective than inferiorly-based flaps for treating VPD because they can be made longer, whereas the length of inferiorly-based flaps is limited by the presence of an adenoid pad. Nonetheless, postoperative acute or chronic complications may occur, including residual VPD, snoring, obstructive sleep apnea (OSA), and even dehiscence. Most complications are acute, occurring within 24 hours postoperatively [1], and Fraulin et al. [2] showed that the overall complication rate decreased from 19.5% to 6.3% during a several-year period.
Previous studies have investigated factors related to the effectiveness of VPD treatment with superiorly-based pharyngeal flaps. Specifically, previous research has explored the associations of the cause of VPD and age at surgery with speech outcomes [3-6]. Some studies have reported that age at surgery was not a critical factor, while others have shown that optimal speech improvements were achieved in younger children [5,7].
In this study of Asian VPD patients, the outcomes of superiorly-based pharyngeal flap surgery performed by a single surgeon were analyzed in terms of postoperative speech outcomes and complications. Speech outcomes were compared according to the cause of VPD and age at surgery.
METHODS
Subjects
Patients treated for VPD from September 1996 to October 2014 were reviewed, and the subjects of this study comprised 72 patients in whom pharyngeal flap surgery was indicated, as confirmed by preoperative speech articulation testing, nasoendoscopy, and lateral video fluoroscopy. An additional inclusion criterion was at least 6 months of follow-up after pharyngeal flap surgery. Surgical complications were evaluated in all 72 patients, and speech outcomes were analyzed in 43 patients for whom speech articulation testing was possible. This study was conducted after receiving approval from the Institutional Review Board (IRB No. 1907-020-081), and all patients (or their guardians) provided informed written consent.
Complications
Acute and chronic complications associated with superiorlybased pharyngeal flap surgery were analyzed in all 72 VPD patients. Acute complications included airway, flap, and donor site problems, whereas chronic complications were determined based on examinations assessing snoring and other respiratory difficulties. For snoring, patients were classified according to whether their symptoms lasted for over 3 months and for over 1 year.
Speech articulation testing
Speech outcomes were evaluated through articulation testing, both preoperatively and at the postoperative follow-up (at 6 months or more). On average, postoperative articulation testing was conducted at 8.5 months after surgery (range, 6ŌĆō24 months). The simple method of evaluating speech in Korean cleft palate patients developed by Kim et al. [8] was used to score their speech. In this method, a total of 22 items are evaluated (hypernasality, five items; plosives, seven items; fricatives, two items; affricates, three items; laterals, two items; and nasal consonants, three items), with a total possible score of 66 points. Five doctors (including a plastic surgery resident) and five medical school students conducted speech articulation testing. PatientsŌĆÖ scores were summed and averaged.
Analysis of speech articulation testing data
The significance of improvements in speech articulation was determined by analyzing the preoperative and postoperative speech articulation test results using the paired t-test. The relationship of the cause of VPD with speech articulation improvement was analyzed using one-way analysis of variance (ANOVA) for five groups (cleft palate, incomplete, cleft palate submucous, cleft lip and palate, complete and idiopathic). The relationship between age at surgery and speech outcomes was also analyzed by one-way ANOVA for four groups (4ŌĆō5 years, 6ŌĆō10 years, 11ŌĆō20 years, and Ōēź 21 years). The p-values were obtained from Mann-Whitney tests conducted as post-hoc tests. This relationship was also quantified by calculating correlation coefficients through linear regression analysis between age at surgery and improvement in the speech articulation test score. Excel 2010 (Microsoft Corp., Redmond, WA, USA) was used for all statistical analyses and p-values < 0.05 were considered to indicate statistical significance except the Mann-Whitney test. p-values < 0.0125 in the Mann-Whitney test using BonferroniŌĆÖs method were considered to indicate statistical significance.
RESULTS
Complications
None of the 72 patients had airway problems immediately after surgery. Nine patients (13%) experienced acute complications at the flap or donor site, including donor site dehiscence in eight patients and pharyngeal flap dehiscence in one patient. Two patients needed at least 2 weeks for complete wound healing. No patients experienced OSA as a chronic complication. However, 35 patients (48%) experienced snoring for more than 3 months after surgery, and snoring lasted for more than 1 year in 16 patients (22%).
The patient who experienced flap dehiscence underwent reoperation using the same surgical technique. Two patients underwent flap division due to ongoing postoperative discomfort, snoring, and hypernasality.
Changes in speech articulation test scores
The average age of the 43 patients for whom it was possible to conduct speech articulation testing was 14.1┬▒ 11.8 years (range, 4ŌĆō52 years). The sex ratio was approximately 1:1 (21 males and 22 females). Preoperatively, the speech articulation test scores ranged from 37.1 to 63.0 (mean, 52.7┬▒ 6.7). Postoperatively, the scores ranged from 42.6 to 66.0 (mean, 59.5┬▒ 5.7). An average improvement of 6.8 points was seen in the speech articulation scores, which was statistically significant (p< 0.05). However, four had slightly decreased postoperative scores.
Association between the cause of VPD and improvements in speech articulation
Incomplete cleft palate was the most common cause of VPD (18 patients). The mean postoperative improvement in speech articulation was highest in patients with submucous cleft palate (10.7 points), but no statistically significant between group difference was found (p= 0.16) (Table 1).
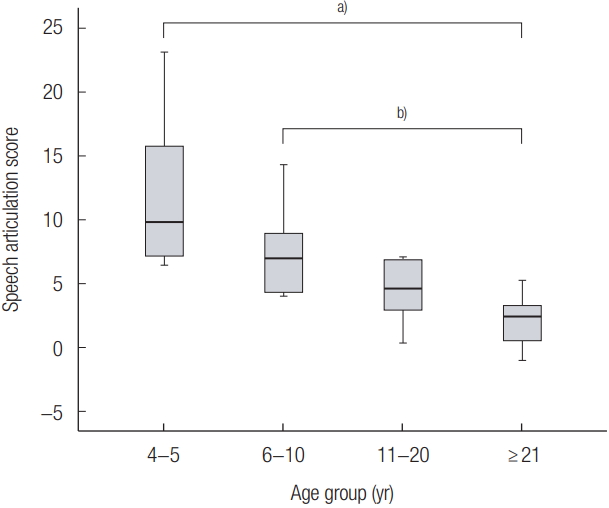
Association between age at surgery and improvements in speech articulation
Statistically significant differences were found between age groups (p< 0.05) (Table 2). The 4ŌĆō5 years group and the 6ŌĆō10 years group exhibited significantly greater improvements in speech articulation testing than the Ōēź 21 years group (MannWhitney test, p< 0.125) (Fig. 1). In addition, age at surgery showed a significant negative correlation with the extent of improvement in speech articulation (p< 0.05) (Fig. 2).
DISCUSSION
Although the success rate of pharyngeal flap surgery for VPD treatment is high, several complications can take place. Respiratory difficulties and flap or donor site dehiscence are examples of acute complications, most of which occur within 24 hours postoperatively. Bleeding, alterations in airway physiology and swelling can cause perioperative airway obstruction, resulting in severe respiratory difficulties that require prompt attention [9]. All patients who experience such complications must receive satisfactory monitoring [9]. We performed real-time saturation monitoring of patients for 24 hours postoperatively to monitor them for the possibility of airway obstruction. Mild breathing difficulties were observed in some patients, but none had severe respiratory difficulties requiring intubation.
Few studies have investigated flap dehiscence after superiorlybased pharyngeal flap surgery. A study reported complete or partial separation of the flap from the palate in up to 7% of cases [10]. Studies have also reported that approximately 3%ŌĆō20% of flaps required revision surgery due to dehiscence [1,11-13]. One patient in our study underwent postoperative endotracheal intubation and was transferred to the intensive care unit due to unanticipated arrhythmia during pharyngeal flap surgery. That patient underwent revision surgery using the same technique.
Chronic complications that occur after pharyngeal flap surgery include OSA and hypernasal speech. OSA has been reported to occur in up to 90% of cases after pharyngeal flap surgery; moreover, since it can potentially cause pulmonary hypertension or right ventricular hypertension, it should be considered as an important complication of pharyngeal flap surgery [1,14-17]. Peat et al. [16] reported that 51% of patients experienced snoring after pharyngeal flap surgery. Two patients in our study underwent a flap division operation due to ongoing discomfort, snoring, and hypernasality caused by persistent nasal obstruction. These patients underwent superiorly-based pharyngeal flap surgery at 10 and 16 years of age, respectively, and complained of persistent nasal obstruction because they perceived the flap as a foreign object. In these patients, flap division surgery successfully resolved their nasal obstruction, and the improvements in speech outcomes that took place after pharyngeal flap surgery were maintained after the division procedure. This may have been because the residual bulk left in the posterior pharyngeal wall after flap division served as a pad to help with velopharyngeal closure, or as a result of the adaptive speech mechanism that the patient learned when the flap was in place [16].
The cause of VPD and the timing of surgery can be considered as possible factors affecting the outcomes of superiorlybased pharyngeal flap surgery in patients with VPD. Some studies have found that the cause of VPD did not significantly affect the extent of improvements in speech articulation after superiorly-based pharyngeal flap surgery [4,6]. Likewise, our study showed postoperative improvements in speech articulation for each cause of VPD, but no significant difference between groups was observed.
Several studies have sought to determine the impact of the timing of surgery on the outcomes of VPD treatment. Some studies have shown that appropriate timing of surgery was associated with a positive impact on improvements in the speech articulation of VPD patients [5,6,18]. However, other studies have shown little effect [3,4]. Dorf and Curtin [19] reported a significant difference in postoperative speech abnormalities in cleft palate patients around 1 year of age. In our study, performing pharyngeal flap surgery at a younger age was associated with greater improvements in speech articulation, supporting other studies that have presented positive reports of performing early surgery in VPD patients, before language development. Early surgery may be especially advantageous for improving postoperative speech articulation in light of recent developments that have shortened the operative time for surgery to treat VPD.
VPD patients who are older than 5 years and have well-developed language habituate to pathological malarticulation that compensates for hypernasality, which is caused by their inability to close the velopharynx. Therefore, delaying surgery for VPD might make the development of malarticulation more likely.
Superiorly-pharyngeal flap surgery is one of many ways to treat VPD. Acute and chronic complications may occur after superiorly-based pharyngeal flap surgery, but most such complications resolve without significant sequelae. In this study, we investigated the cause of VPD and the timing of surgery as factors that may affect the outcomes of superiorly-based pharyngeal flap surgery in VPD patients. Significant postoperative improvements in speech outcomes were observed, but with no significant difference according to the cause of VPD, consistent with previous studies. We also investigated the most appropriate timing of surgery for VPD patients, and found that performing surgery at a younger age led to better speech outcomes. In addition, the superiorly-based pharyngeal flap was a successful way to improve speech outcomes in VPD patients, especially those who were younger.
Potential limitations of this study include the fact that it analyzed a small number of patients, especially given the lack of other studies in the literature on additional factors that may influence speech outcomes after superiorly-based pharyngeal flap surgery. Nevertheless, our study is noteworthy in that it makes a novel contribution to the relatively sparse literature on superiorly-based pharyngeal flap surgery in patients with VPD.