INTRODUCTION
Reconstruction for tissues of the head and neck region that are altered by any cause must consider the functional aspects, including respiration, mastication, swallowing, and vocalization, as well as the cosmetic appearance. With recent advances in microsurgery, free-flap reconstruction has become the first-line treatment for head and neck reconstruction because it can improve both functional and cosmetic aspects using tissues from different sites with features similar to those of the defect site. The flap survival rate of head and neck reconstruction using free flaps is reported to be approximately 95%ŌĆō98% [1,2]. Moreover, deficits that require free-tissue transfer are related to the tumor resection in > 97% of the cases [2].
Recurrent tumor at the primary site occurs in approximately 20%ŌĆō30% of patients with head and neck cancer and remains the most common cause of treatment failure [3-6]. Management of recurrence after surgical resection is challenging. Treatment options include salvage surgery, radiation, chemotherapy, a combination of these therapies, and palliative care. Most head and neck oncologists agree that salvage surgery would provide the best chance of long-term disease control and possible cure for patients with resectable recurrent cancers [4-8]. However, salvage reconstruction for recurrent head and neck cancer may be more challenging because of previous treatment, which may include chemotherapy, radiation, neck dissection, and free-flap reconstruction. Radiotherapy could result in scarring and neck tissue fibrosis [9]. Patients who undergo neck dissection lack potential recipient vessels and have periadventitial scarring and perioperative thrombosis of major vessels [10]. If they had previously undergone free-flap reconstruction, the neck dissection can lead to technical difficulties and a higher chance of tissue damage [11].
Hence, this study aimed to investigate whether previous treatments affect the survival rate of free-flap reconstruction and influence the selection of recipient vessels during salvage surgery using free flaps in patients with recurrent head and neck cancer.
METHODS
Of a total of 830 cases of free-flap reconstruction in the head and neck region from 1993 to 2017, the medical records of 124 (116 patients) free-flap reconstructions for recurrent head and neck cancer were investigated in this retrospective study. For comparison, 643 patients (647 cases) who had free-flap reconstruction for primary head and neck cancer were assigned to a control group. All of the reconstructive operations were performed by a single experienced reconstructive team to minimize the effects of the learning curve and measurement bias.
Previous treatments included radiotherapy, chemotherapy, concurrent chemo-radiotherapy, wide mass excision excluding neck dissection, wide mass excision including ipsilateral or bilateral neck dissection, and free-flap reconstruction.
Vascular crises were classified according to the cause, which included venous congestion, arterial insufficiency, and carotid blowout. Revision and flap failure cases were categorized according to attempted versus not attempting salvage, and the success rate was confirmed based on the eventual survival of the flap. The total flap success rate of the recurrent cancer group was compared with that of the primary cancer group, and the difference was analyzed in relation to whether the patients in the recurrent cancer group received a previous treatment. Moreover, the incidence of postoperative infection was evaluated. Infections were classified as either major, which require an operation; or minor infection, which are managed conservatively.
The recipient vessel used in the free-flap reconstruction was identified, and the cases in the recurrent cancer group were categorized into ipsilateral and contralateral anastomosis. If the conventional method could not be performed, such that the common carotid trunk or vein graft was used, the case was categorized as an uncommon anastomosis. Analysis of the classified recipient vessel group was performed to determine whether differences exist according to history of neck dissection. Pearson chi-square test and analysis of variance were performed, with the significance level set at p< 0.05. All statistical analyses were conducted using SPSS version 25.0 (IBM Corp., Armonk, NY, USA). This study was approved by the appropriate institutional review board and performed in accordance with the principles of the Declaration of Helsinki. Written informed consent was obtained.
RESULTS
The mean age of the patients was 56.6 years. Of the 124 patients, 94 were male and 30 were female. The primary tumor site included the oral cavity (45 cases), oropharynx (23 cases), maxilla (18 cases), larynx (15 cases), hypopharynx (10 cases), nasopharynx (6 cases), submandibular gland (4 cases), parotid gland (1 case), upper lip (1 case), and thyroid gland (1 case). In terms of histological classification, 107 cases were squamous cell carcinoma, 12 were adenoid cystic carcinoma, two were fibromyxoid sarcoma, one was papillary carcinoma, one was verrucous carcinoma, and one was malignant melanoma. Regarding cancer staging, 73 cases were T4, 16 were T3, 19 were T2, 12 were T1, and four were T0. The type of free-flap used for salvage reconstruction was radial forearm (52 cases), anterolateral thigh (48 cases), fibula osteocutaneous (11 cases), rectus musculocutaneous abdominis (7 cases), latissimus dorsi musculocutaneous (6 cases) (Table 1).
Of the 124 cases, 89 (71.8%) had undergone radiotherapy and 69 (55.6%) neck dissection (ipsilateral in 40 and bilateral in 29) as the previous treatment. Free-flap reconstruction was performed in 40 (32.3%) (Table 2), including radial forearm (25 cases), anterolateral thigh (12 cases), fibula osteocutaneous (1 case), and rectus abdominis musculocutaneous free flaps (2 cases) (Table 3).
The type of free-flap used for the salvage reconstruction was radial forearm (52 cases), anterolateral thigh (47 cases), fibula osteocutaneous (11 cases), latissimus dorsi musculocutaneous (5 cases), rectus abdominis musculocutaneous (7 cases), and jejunal (1 case). In one case, anterolateral thigh and pectoralis major musculocutaneous pedicled flaps were simultaneously used for reconstruction of the primary cancer site (Table 4).
The success rate of free-flap reconstruction in patients with recurrent head and neck cancer was 95.2%. Ten cases (8.1%) of vascular crisis were noted: five cases of venous congestion, two cases of arterial insufficiency, and three cases of carotid artery blowout. Moreover, revision was performed in six of the 10 cases, with successful salvage in only four. Thus, a total of six cases (4.8%) had total flap failure (i.e., 4 where revision was not possible and 2 with failed revision). The success rate in the control group, i.e., the patients with primary head and neck cancer, was 98.8%; of 647 cases, only eight (1.2%) developed total flap failure. A statistically significant difference in success rates between the control and recurrent cancer groups was observed (p= 0.006).
The analysis examining the association of vascular crises with previous radiotherapy, neck dissection, or free-flap reconstruction demonstrated no statistically significant relationship (p> 0.05) with any of these treatments (Table 5).
Postoperative infection occurred in 51 cases (41.1%), with 30 being major infections requiring an operation. The operations performed included incision and drainage (4 cases), debridement and closure (8 cases), skin grafting (3 cases), pedicled flap reconstruction (8 cases), additional free-flap reconstruction (2 cases), and pharyngostoma formation (1 case). Moreover, two cases of vascular revision for carotid blowout due to infection were successfully salvaged, while two patients who developed systemic infection, which required various operative procedures, died. Minor infection occurred in 21 cases and was treated conservatively.
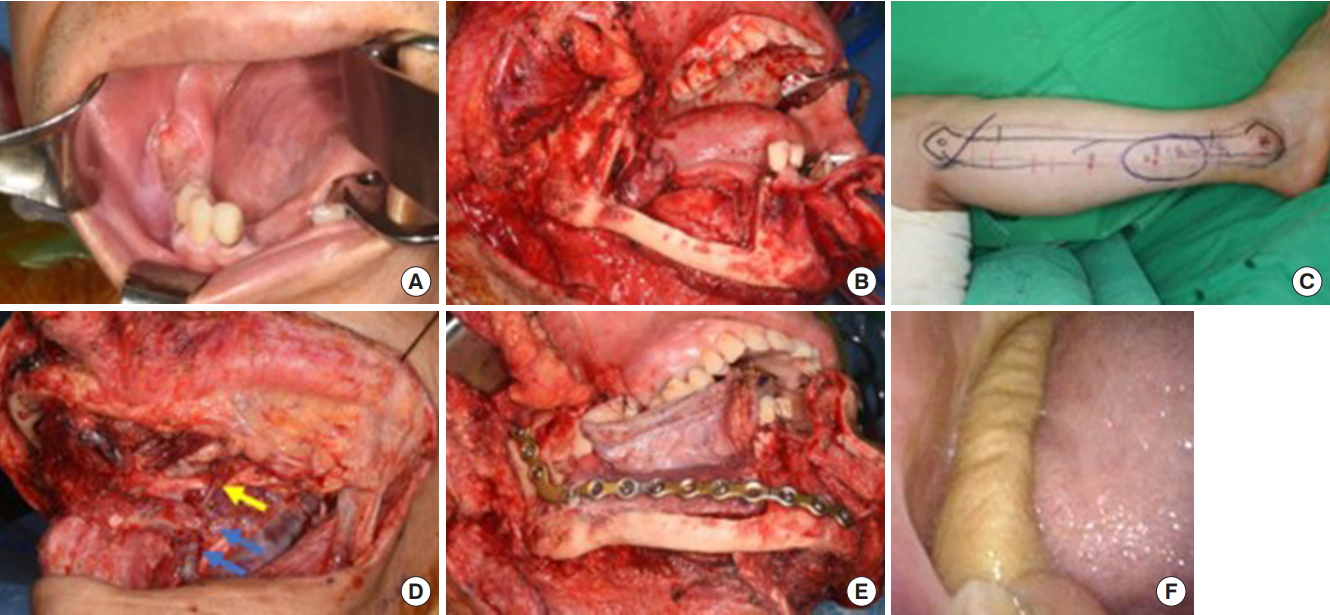
We further evaluated whether a previous neck dissection influenced the selection of the recipient artery for arterial anastomosis. Seventy-three patients received an anastomosis between the primary tumor site and the ipsilateral neck artery, of which 27 had undergone previous neck dissection and 46 had not. Twenty-nine patients received a contralateral side anastomosis (Fig. 1), of which 23 had undergone previous neck dissection and six had not. Moreover, 19 patients had a direct anastomosis of the artery to the common carotid trunk as the conventional recipient vessel could not be used (Fig. 2), and three involved a vein graft for the venous anastomosis (Fig. 3). There were no cases of vein graft use for the arterial anastomosis. Of the 22 cases of uncommon anastomosis, 19 were in patients that had undergone neck dissection and only three were in those that had not. Statistical analyses confirmed that a higher percentage of reconstructions in patients with a previous neck dissection involved contralateral or uncommon anastomoses (p< 0.05).
DISCUSSION
Whether previous treatments could influence surgical outcomes of salvage reconstruction for recurrent head and neck cancer remains to be clearly established. In this study, we found no significant effect of previous treatments, such as radiotherapy (p= 0.897), neck dissection (p= 0.78), or free-flap reconstruction (p= 0.585), on the overall flap survival rate. This finding is consistent with the results of previous studies [9-16]. Nevertheless, a statistically significant difference (p= 0.006) in the success rate of free-flap reconstruction was observed between the control group (98.8%) and the recurrent cancer group (95.2%). This could be explained by the fact that complicating factors (i.e., multiple comorbidities, advanced cancer stage, postoperative infection, or poor general condition) may have affected the outcome of patients in the recurrent cancer group, despite the little influence of a particular previous treatment on overall flap survival. In previous studies, the success rate of free-flap reconstruction for recurrent head and neck cancer was approximately 92%ŌĆō96% [9,11-13,15]; thus, the flap survival rate of 95.2% in our study seems to be a comparatively reasonable outcome.
A considerable difference in the selection of the recipient artery was found between those with and those without previous neck dissection. A tendency to perform the arterial anastomosis at the contralateral side was noted in the 60.8% of patients who had previous neck dissection (p< 0.05), which is in agreement with the finding in previous studies. Head et al. [10] demonstrated that in patients with previous neck dissection, the recipient vessel is located at the contralateral side in approximately 61% of cases. Tan et al. [16] also found a statistical significance in the frequent selection of contralateral neck vessels during neck dissection.
Furthermore, 22 cases of uncommon anastomosis were analyzed, of which 19 had end-to-side arterial anastomosis at the carotid trunk and three used vein grafts for venous anastomosis. No cases involved a vein graft for arterial anastomosis, owing to the fact that when the pedicle is short, end-to-side arterial anastomosis is performed at the ipsilateral carotid trunk to reduce the usage of vein grafts, and that venous anastomosis is inevitably performed when using vein grafts to connect the opposite side. Based on the results of the statistical analysis in our study, previous neck dissection increased the frequency of contralateral side anastomosis as well as unconventional procedures, such as direct carotid trunk anastomosis or vein grafting (p< 0.05). Although a previous study reported a few cases of end-to-side anastomosis at the carotid artery, our study is the first to consider the actual clinical significance [10].
In this study, four vein grafts were used for the venous anastomosis in three cases; however, neither flap failures nor revisions were observed. Nevertheless, numerous studies reported that using a vein graft for free-flap reconstruction could increase vascular compromise and cause flap failure [10,17,18]. Some studies recommended cephalic vein transposition in lieu of a vein graft if there is no recipient vein in the neck region [2,10,15]. However, Furr et al. [19] showed that various factors, such as radiation therapy, prior neck dissection, and prior freeflap reconstruction, could increase the demand for vein grafts; nevertheless, whether the use of a vein graft could independently influence flap survival remains unclear. Furthermore, Hanasono et al. [14] suggested that a vein grafts only be used when absolutely necessary and that extremely lengthy grafts be avoided.
Mucke et al. [20] stated that previous neck dissection could affect microvascular revision and could result in total flap failure, which could be attributed to inadvertent vascular injury and ligation of potential recipient vessels. However, the authors failed to mention whether significant differences in the use of neck vessels (i.e., ipsilateral or contralateral) between those with and those without neck dissection were found. Instead, they recommended that the use of contralateral neck vessel be avoided because it could prolong the duration of the operation, the additional dissection in the opposite neck could increase the risk of morbidity, and the risk of kinking or compression of the vein may increase as the length of the vascular pedicle becomes longer.
Postoperative infection occurred in 51 cases (41.1%), with 30 being major infections requiring an operation. We believe that this is because patients that develop recurrent cancer and multiple comorbidities become more vulnerable to infection, require long operation times due to this being a secondary procedure, and receive pre- or postoperative radiotherapy or chemotherapy, which can result in immunosuppression. Hence, free-flap reconstruction in patients with recurrent cancer must carefully consider their preoperative status and the history of infection. Moreover, during the operation, aseptic techniques should be strictly observed and prolonged operations avoided. Following the operation, signs of infection should be monitored and appropriate antibiotics must be prescribed; proactive infection control could be achieved by operative intervention, if necessary.
The time to recurrence after treatment of the primary cancer ranged from 2 to 180 months, with an average of 33.2 months. The average time of recurrence according to the primary tumor site was 29.9 months for oral cavity tumors, 35.2 months for oropharynx tumors, 35.7 months for maxilla tumors, 32.3 months for larynx tumors, 34.7 months for hypopharynx tumors, 35.3 months for nasopharynx tumors, and 28.8 months for submandibular gland tumors. There was no significant difference according to the primary site (p> 0.05). In terms of histologic type, the average time to recurrence for squamous cell carcinoma was 31.4 months while that for adenoid cystic carcinoma was 38.3 months. There was no significant difference according to cancer histology (p> 0.05).
Based on the results of this study, the following strategies for salvage reconstruction using free flaps in patients with recurrent head and neck cancer could be applied: if the patient had undergone previous neck dissection that resulted in severe periadventitial scarring or perioperative thrombosis in the ipsilateral neck vessel, the contralateral vessel should be utilized. In such cases, a flap with a long vascular pedicle should be used, if possible, to reduce the use of vein grafts; however, a vein graft may be inevitable in some cases. Moreover, if there is no suitable contralateral vessel, end-to-side anastomosis at the carotid trunk could be attempted. In addition, if a single free-flap reconstruction does not provide enough coverage, especially in cases with a large volume deficit or multiple defects, a concurrent pedicled flap, such as pectoralis major musculocutaneous or latissimus dorsi musculocutaneous flaps, could be considered. As there is a high chance of surgical site infection, appropriate pre- and postoperative management is critical. Infection could result in vascular crises, such as carotid blowout; thus, careful management is essential.