INTRODUCTION
It is rare for two different types of skin cancers to occur concurrently in the same area [1]. A collision tumor is a combination of two types of tumors in a single lesion [2]. Collision tumors rarely occur in the skin. The malignant-benign tumors of a different origin from the single tumor are the most common type of collision tumors followed by the benign-benign tumors; collision tumors composed of malignant-malignant tumors case are rare [3]. When two types of malignant tumors develop concurrently in the same area, the combination of malignant melanoma and basal cell carcinoma (BCC) is most commonly observed. According to several articles, the prevalence of collision tumors is very low. Especially, the combination of BCC and squamous cell carcinoma (SCC) was rarely found [4]. Here, we report a case of BCC and SCC in a single tumor in the anterior auricular area in a 70-year-old woman detected on histological analysis.
CASE REPORT
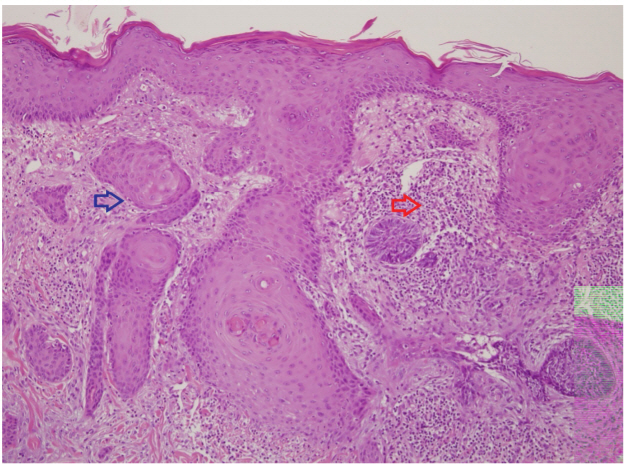
A 70-year-old woman presented with a tumor on the left anterior auricular area. the tumor appeared in the left anterior auricular area one month before a visit to the dermatology clinic. The patient was then diagnosed with BCC based on a punch biopsy. She was transferred to our department to undergo excision of BCC. There were no specific findings in the past and family history. A mass was approximately 1.6├Ś1.4 cm in size, triangular in shape and firmly fixed to the anterior auricular area. The surface of the mass was reddish and there is an ulcer in the center with irregular boundaries (Fig. 1). The patient underwent complete resection with 3 mm safety margin and primary closure under local anesthesia (Fig. 2). The biopsy of the excised specimens revealed no carcinoma in the resection margin, and both BCC and SCC were diagnosed. On histopathologic examination, typical SCC has nests of squamous epithelial cells arising from the epidermis, extending into the dermis and forming keratin pearls on the left side of the hematoxylin and eosin stained specimen observed under a magnification of ├Ś100. In addition, SCC was well-differentiated and had clear margins. On the right side of the specimen, BCC cells were observed where basaloid epithelium was clearly separated from SCC and typically formed palisades. These two cell types were clearly separated from each other rather than being observed together in a single tumor cell, as observed in basosquamous carcinoma (Fig. 3). There has been no recurrence or metastasis to date, and we continue to follow-up the patient for 1 year.
DISCUSSION
A collision tumor is a combination of two types of tumors in a single lesion [2]. The pathogenesis of collision tumors is a matter of speculation [5]. Some authors consider the pathogenesis of collision tumors to be coincidental [6]. Other hypothesis is that one tumor induces epithelial or stromal changes to develop second tumor [7]. Collision tumors rarely occur in the skin. collision tumors composed of malignant-malignant tumors case are rare [3]. In particular, the BCC and SCC are rare.
In this report, we discuss a rare case of BCC and SCC in a single tumor that was successfully treated by wide excision of the tumor. BCC and SCC in a single lesion are the most common skin cancers observed by plastic surgeons. Although there are some outpatients who visit the clinic directly, most patients present to the plastic surgery department after being diagnosed with skin cancer based on punch biopsy findings at a dermatology clinic. In most cases, a treatment plan is established based on the results of a biopsy. The present case illustrates that two types of skin cancer, BCC and SCC, can occur in a single lesion.
From the viewpoint of a plastic surgeon, the accurate diagnosis of BCC and SCC is important. Accurate and complete treatment according to the type of skin carcinoma is also important. The most familiar and facile technique for the treatment of BCC and SCC is surgical excision. Currently, BCC and SCC differ in terms of recommended excision margins for complete excision. Therefore, it is important to determine surgical treatment following accurate diagnosis of BCC and SCC.
First, with respect to BCC, the goal of the treatment is to perform complete excision by establishing appropriate surgical margins. Although there are some inconsistencies regarding the surgical margins among studies, excision with 3-mm margins is generally recommended for small and well defined primary BCCs [8-13]. According to a study, 2-mm margins are sufficient in some cases [11,14].
In the case of SCC, surgical excision should include normal skin margins and subcutaneous fat for complete excision [15,16]. With respect to the appropriate surgical margins, lowrisk SCCs require 4-mm margins, and high-risk SCCs require 6-mm margins [17].
Other treatments include cryotherapy, electrodesiccation, 5-FU (5-fluorouracil), radiation therapy and Mohs micrographic surgery. The prognosis and treatment of these cases are dictated by the more serious tumor. When diagnosed early and excised with the recommended margins, the prognosis seems to be good as in this patient.
Therefore, it is important to always consider the possibility of composite tumors, carefully perform a punch biopsy of the suspected carcinoma before diagnosis, and obtain frozen sections during surgery to determine appropriate surgical margins according to the biopsy results.
With respect to histologic findings, BCC and SCC were observed as being clearly separate from each other when the specimen was observed at a magnification ├Ś100. However, it is difficult to completely disregard the possibility of SCC differentiating into basosquamous carcinoma where squamous carcinoma cells may be invisible around the basal carcinoma cells. Furthermore, this tumor may be a basosquamous carcinoma, a subtype of BCC, and not a collision tumor. However, the pathologic findings showed that the two types of cancer cells were separated; therefore, it is very unlikely that this was a basosquamous carcinoma.
In conclusion, BCC, SCC, and basosquamous cell carcinoma differ in terms of prognosis, risk of metastasis, and the recommended surgical margins for complete excision; accurate differential diagnosis is necessary, and appropriate treatment and follow-up are needed. Therefore, when determining the diagnosis and surgical treatment of patients with skin cancer, we should not rule out the possibility that BCC and SCC may coexist and that basosquamous cell carcinoma may develop even if patients are referred to plastic surgeons after being diagnosed with BCC and SCC in other hospitals or dermatology clinics.