INTRODUCTION
Sclerotic fibroma of the skin is a rare fibrous tumor of the skin. The two types of sclerotic fibromas are known as multiple lesions associated with CowdenŌĆÖs disease [1], and solitary lesions without CowdenŌĆÖs disease [2]. Solitary sclerotic fibroma is rare and extremely difficult to diagnose based on clinical findings only because these findings are nonspecific and similar to keloid scar. We have experienced a case of solitary sclerotic fibroma at the left lateral thigh area in a 25-year-old man, which the clinical findings were similar to a keloid scar. Therefore, a careful approach to clinical and histological examination is required for patients with these similar lesions.
CASE REPORT
A 25-year-old man presented to our hospital with a mass on the left thigh, which he had for 2 years. Clinical assessments at the first visit revealed a firm, fixed, well-circumscribed, pinkish polypoid tumor measuring about 3├Ś3├Ś1.5 cm (Fig. 1). He was in the habit of picking pieces of the small mass from time to time. There was no specific family history or past medical history related to solitary sclerotic fibroma and physical examination showed neither pain nor tenderness. Under general anesthesia, the authors performed a surgical excision and the defect was covered with a split thickness skin graft without radiation therapy (Fig. 2).
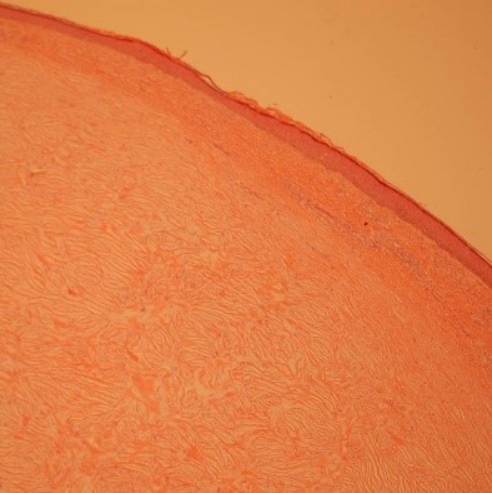
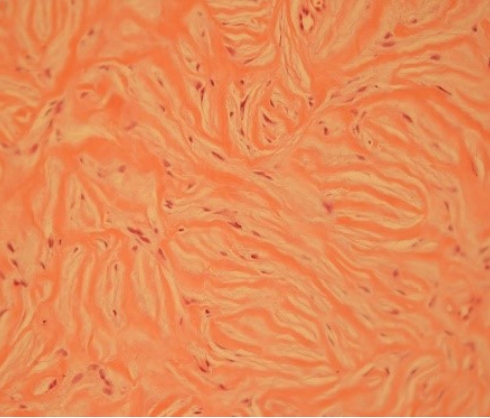
Histopathologically, the lesion showed a wellŌĆÉdefined, hypocellular intradermal fibrotic nodule (Fig. 3). It was negative for CD 34, smooth muscle actin, ╬▓-catenin and showed abundant, dense hyalinized collagen bundles (Fig. 4). The most central area had a storiform arrangement intermixed with paucicellular dense collagen bundle that were separated by prominent clefts and it was consistent with sclerotic fibroma (Fig. 5).
DISCUSSION
Sclerotic fibromas were first reported in 1972 by Weary et al. [1] as multiple tumors in the tongue of patients with CowdenŌĆÖs disease. In 1989, Rapini and Golitz [2] reported 11 cases of similar sclerotic fibromas in patients without CowdenŌĆÖs disease and were called solitary sclerotic fibroma. The mean patient age was 40 years with a range of 7 to 62. There was no preferential location; however, five of 11 lesions were located in the head and neck region. The lesion was more common in females (8 of 11). The average lesion size was 5.5 mm with a range of 2 to 9 mm. Since our case did not satisfy the diagnostic criteria of CowdenŌĆÖs disease, the patient was diagnosed with a solitary sclerotic fibroma. Clinically, solitary sclerotic fibroma presents as asymptomatic, well-defined, skin-colored, round to ovoid nodules. Because the clinical findings were similar to a keloid scar, it was difficult to confirm the diagnosis. Therefore, it is important to differentiate between sclerotic fibroma and keloid scar to determine the treatment model for prevention of recurrence after surgery.
Sclerotic fibroma is commonly found on the face and limbs but it also appears on the scalp, trunk, and oral mucosa [3,4]. It presents as slow-growing flesh-colored papule or nodule and has an excellent prognosis.
Alternatively, the common sites of keloid scars are the earlobe, presternal, and deltoid regions. They often have a definite trauma history. It presents as a scar or mass that grows beyond original wound and recurrence are relatively common. Therefore, surgical excision alone has an excessively high recurrence rate. Radiation therapies have been known to reduce the recurrence rate of keloid scar [5,6].
Sclerotic fibroma should be considered in the differential diagnosis with keloid scar and histopathology is the most reliable method to confirm the diagnosis. A sclerotic fibroma shows paucicellular dense and relatively thin collagenous bundles that are separated by prominent clefts arranged in a storiform pattern, while a keloid scar show dense, broad, haphazardly arranged thick collagen bundles which exhibits a ripple-like arrangement (Table 1).
In summary, sclerotic fibroma is a relatively rare soft tissue tumor of the skin that shows characteristic histopathological findings but nonspecific clinical findings. Although the clinical appearance is indistinct, the histopathological characteristics are firmly established and easily recognized. Surgeons should include sclerotic fibroma in the differential diagnosis of keloid scar and histopathology is needed to confirm the diagnosis.