INTRODUCTION
Basal cell nevus syndrome (BCNS) is a rare disease inherited in an autosomal dominant manner. It is characterized by the development of early-onset basal cell carcinomas [1,2]. The pathogenesis of BCNS is primarily associated with mutations in the PTCH1 gene and rarely associated with mutations in the suppressor of fused and PTCH2 genes [3,4]. The BCNS was first reported by Jarisch [5], who described a patient with multiple basal cell carcinomas in 1894. Gorlin and Goltz first defined this condition as an autosomal dominant syndrome, comprising the principal triad of basal cell carcinoma, jaw cysts, and bifid ribs [5,6]. The prevalence of BCNS ranges from 1/57,000 to 1/256,000 and has a male to female ratio of 1:1. It has a lower prevalence rate of one per 13.9 million in Korea [2,7-10]. In this case report, we described our experience with a patient who presented with basal cell carcinomas and was diagnosed with BCNS.
CASE REPORT
A 40-year-old man visited the hospital with multiple non-tender masses on his face present for a long time. According to the patient, the masses began to appear on his face and neck 25 years ago, and some were diagnosed as basal cell carcinoma. The mass was evaluated using computed tomography (CT) and positron emission tomography-CT, but the results were nonspecific. Therefore, we decided to perform surgical excision under the initial impression of multiple basal cell carcinomas. Under general anesthesia, 59 lesions were removed (Figs. 1, 2). Histology of the 59 lesions showed that all, except five lesions, tested positive for basal cell carcinoma.
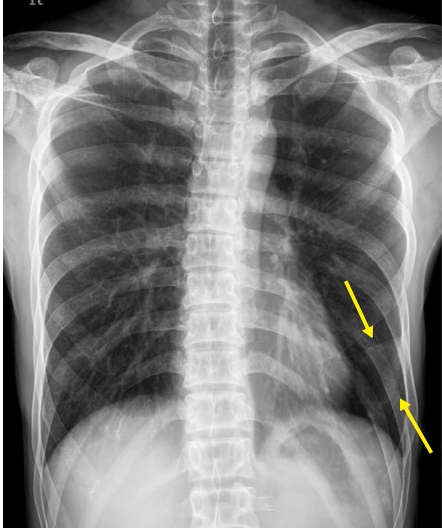
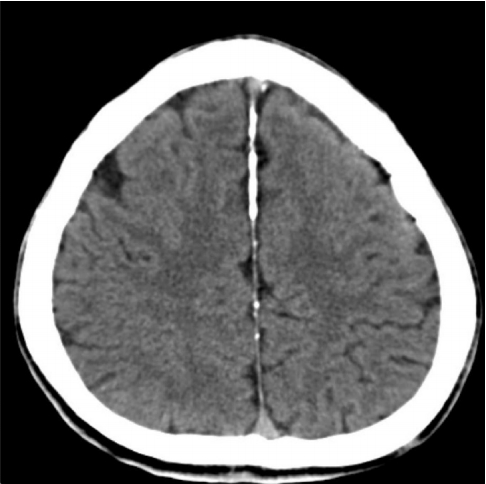
Based on the biopsy results, we suspected a BCNS (Fig. 3). Therefore, the patientŌĆÖs family history, personal history, and radiographic examinations were reviewed. He had a history of excisional surgery for his jaw cyst, which was diagnosed as an odontogenic keratocyst when he was 19 years old. The suspected odontogenic cyst was identified through a panoramic view (Fig. 4). A bifid left sixth rib was observed on the anteroposterior view of the chest radiograph (Fig. 5), and brain CT revealed extensive calcifications of the falx cerebri (Fig. 6). He was diagnosed with BCNS based on findings matching the diagnostic criteria for BCNS [11].
The postoperative course was uneventful, and there was no recurrence or complications during the 10-month follow-up period. Although we recommended genetic tests of the patient and his relatives for more comprehensive treatment, the patient and the relatives declined to do so.
DISCUSSION
BCNS is a rare multisystemic disease inherited in an autosomal dominant condition with variable penetrance and its development was mainly associated with variations in the PTCH1 gene [6,7]. PTCH1 regulates the growth of normal tissues and produces a tumor suppression factor [3].
The prevalence of BCNS is approximately one in 57,000 to one in 164,000 [1]. Men and women are equally affected [9]. In Korea, few cases of BCNS have been reported, and the reported prevalence of BCNS is approximately one in 13,939,393 [10].
BCNS is associated with different signs and symptoms. As the name suggests, the most common symptom of BCNS is the early development of basal cell carcinomas. While basal cell carcinomas are generally known to occur at over 60 years of age, basal cell carcinomas in BCNS are known to develop between puberty and 35 years of age [3,12]. Additional clinical features include odontogenic keratocysts, palmar and plantar pitting, frontal bossing, skeletal anomalies such as bifid ribs, Sprengel deformity, deformity of the pectus, polydactyly, syndactyly, hypertelorism, medulloblastoma or fibroma of ovaries, and lamellar calcification of the falx cerebri [3,13]. Since medulloblastoma can cause early death, BCNS patients must undergo immediate screening so they can be diagnosed promptly [1,3].
Evans et al. first introduced the diagnostic criterion for BCNS, based on the most frequent and distinguishing clinical characteristics in 1993. This was updated in 1997 by Kimonis et al. [1] and in 2011 by Bree et al. [11]. These criteria have been continuously refined, but a final consensus has not been reached. In general, BCNS can be diagnosed if two major criteria or one major criterion and two minor criteria are met [3]. Recently, a new diagnostic condition of one major criterion with molecular confirmation has been introduced [11]. In our case, we were able to identify three major clinical features, including basal cell carcinomas, odontogenic keratocysts, and calcification of the falx cerebri. Bifid rib, which is a minor clinical symptom, was also observed. The patient was diagnosed with BCNS. The patient and his relatives declined to undergo genetic testing which was considered essential to obtain precise genetic confirmation.
The treatment of BCNS requires a multidisciplinary approach due to its various clinical manifestations. Although various treatments for BCNS have been suggested, no ideal treatment exists, and previous studies have focused on surgical excision using the standard or Mohs technique [13]. In our case, the basal cell carcinomas were managed with surgical excision by establishing appropriate surgical margins [14], and these did not recur during the observation period. However, periodic dermatologic examinations are necessary for BCNS patients to check for the possibility of recurrence.
In summary, BCNS is a rare disease that is difficult to diagnose and treat early. If suspected, various tests should be conducted at an early age, and accurate treatment is possible only when experts in various fields have adequate knowledge of BCNS. In addition, family members of patients diagnosed with BCNS should undergo genetic testing because of the genetic relevance of BCNS.