INTRODUCTION
Fibrofolliculoma is an autosomal dominant benign tumor characteristically found alongside the Birt-Hogg-Dube syndrome, involving trichodiscoma, acrochordon, multiple fibrofolliculomas, and internal neoplasms [1]. Most fibrofolliculomas are smooth papules with a dome shape, size of 2ŌĆō4 mm, and with multiple lesions occurring around the face [2]. Solitary fibrofolliculomas are rare. In 1984, Scully et al. [3] were the first to report a case of solitary fibrofolliculoma without genetic tendency and other skin lesions. However, only few cases have been reported since then. To the best of our knowledge, only 14 cases have been reported, of which two occurred in the nose (Table 1). However, none of these cases occurred in the alar rim [1,4-6]. Fibrofolliculoma is a rare disease, and it occurs either as multiple lesions or in association with genetic diseases such as Birt-Hogg-Dube syndrome; therefore, solitary fibrofolliculoma without other cutaneous abnormalities is extremely rare in clinical practice. Histological examinations have revealed the lesions to be clinical entities that lie somewhere between perifollicular fibroma and trichofolliculoma [7]; therefore, it is very difficult to distinguish these lesions from other pathologies. We herein present a case of a solitary fibrofolliculoma occurring in the alar rim of a healthy male and describe the treatment process and the pathology results.
CASE REPORT
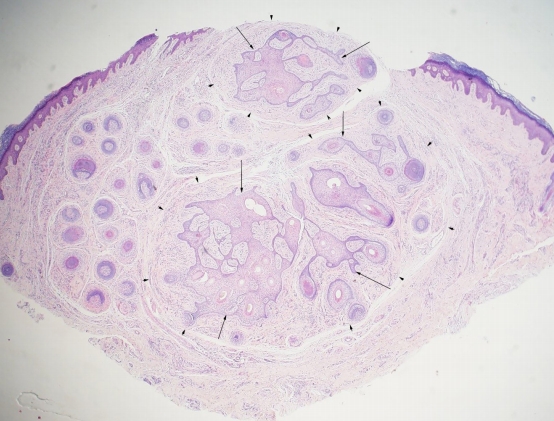
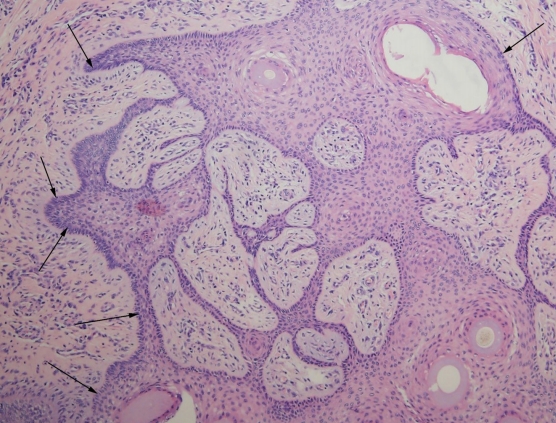
A 42-year-old man presented to the hospital with a palpable mass, which had appeared a year ago, on his left alar rim (Fig. 1). The mass was 5├Ś 7 mm in size, protruding and palpable, dome shaped, and the same color as that of his skin. He did not have similar lesions in other areas of his body. In addition, none of his family members were known to have such a lesion. The patient had visited a local hospital before consulting in our clinic and had been diagnosed with keratoacanthoma. Under this diagnosis, incisional biopsy was performed on a portion of the mass for histological confirmation, along with the removal of the lesion. Pathologic examination revealed hyperkeratosis and parakeratosis, and complete excision was planned. Under local anesthesia, an elliptical incision was made to remove the lesion, including the mass. When viewed with the naked eye, no invasion of the mass into cartilage or other tissues was observed, and no adhesion to the periphery was observed. Therefore, the mass was considered to have been completely excised above the perichondrium. Permanent biopsy was requested for the excised mass, and nevus sebaceous was confirmed. We requested the pathology department for a review because it did not seem clinically correct, as nevus sebaceous is a congenital malformation that can be found on the face [12]. Histological examination revealed the presence of proliferative follicular epithelium surrounded by perifollicular fibrous tissue (Fig. 2). Thin epidermal strands originated from the hair follicles and centered around the infundibulum of the hair. The connective tissue around the epithelium also showed sclerotic features (Fig. 3). Based on these pathological results, the final diagnosis was fibrofolliculoma.
DISCUSSION
Several tumors are formed in hair follicles [13-16]. Clinically, it is very difficult to distinguish fibrofolliculoma from trichodiscoma and perifollicular fibroma. When viewed with the naked eye, all these lesions are pale-yellow or white, 2ŌĆō4 mm in size, usually dome shaped, and smooth [3]. Furthermore, according to the cases of solitary fibrofolliculoma reported thus far, most of them occurred in patients aged 50 years or older, and unlike multiple fibrofolliculomas, they do not show a genetic tendency and do not accompany other skin diseases [5]. To date, the only method for obtaining a definitive diagnosis of fibrofolliculoma is pathology. Therefore, diagnosis is made according to the pathological examination of an incisional biopsy and clinical judgment at presentation. In addition, solitary fibrofolliculoma is very rare; hence, there are not many clinical cases, and because it is difficult to distinguish between clinically similar types of perifollicular fibromas and trichodiscomas, it is highly likely to be misdiagnosed. Therefore, biopsy should be performed. Histologically, fibrofolliculoma is represented as a circular or oval-shaped well-bounded fibroepithelial proliferative tumor in the dermis, which appears as a concentric circle around the hair follicle. In the center of the tumor, epithelial proliferation of a single follicular infundibulum is generally observed and forms an epithelial zone that extends into the surrounding fibrous matrix, leading to unique network formation by anastomosis [8,17]. In this case, the lesion had thin epidermal strands centered around the infundibulum of the hair and the proliferative follicular epithelium, surrounded by connective tissue. In the case of multiple fibrofolliculomas, laser therapy using Erbium-YAG or CO2 and systemic isotretinoin administration are reportedly effective; nevertheless, treatment results vary [18]. Because of their rarity, there is no consensus on the treatment and prognosis of solitary fibrofolliculoma. Even though solitary fibrofolliculoma is known to be a benign mass, complete resection is considered desirable. In addition, as the protruding mass changes the shape of the alar rim, it was judged that complete resection is more desirable than other treatment methods to provide the patient a contouring effect for esthetic purposes. We report the diagnosis and treatment of a solitary fibrofolliculoma, a rare disease, in a healthy male with no specific medical history or family history of mass development in the nose. Fibrofolliculoma is a rare disease; however, when a mass occurs in the nose, clinicians should suspect fibrofolliculoma based on the clinical and histological characteristics presented in this case and consider treatment based on diagnostic tests and complete resection.