Clinical characteristics of adolescent nasal bone fractures
Article information

Abstract
Background
There have been many reports of nasal bone fractures in adults, but there are few clinical reports of them in adolescents, although adolescence is the main growth period of the nasal bone. In addition, previous studies have tended to classify and describe child and adolescent nasal fractures in the same category. The aim of this study was to identify the clinical aspects of nasal fractures in adolescents, and to evaluate the characteristics of nasal fractures in the growth period.
Methods
Our institution’s database was reviewed to extract data on adolescent patients between the age of 13 to 18 who had isolated nasal bone fractures from March 2012 to February 2020. The study excluded patients with other facial fractures, previous facial fractures, or congenital deformities.
Results
This study included 243 boys and 26 girls. Interpersonal violence and sports-related accidents accounted for 85 and 79 cases, respectively. There were 128 frontal impact injuries and 132 lateral impact injuries, and 97 patients had accompanying septal fractures. An accompanying septal fracture was present in 36.06% of all patients, but in 51.20% of those who underwent surgery.
Conclusion
The prevalence of adolescent nasal fractures was significantly higher in boys, to a greater extent than observed for pediatric or adult fractures. The main causes of fractures were interpersonal violence and sports-related accidents. An explanation for these results is that adolescent boys are more prone to have violent accidents or companionship with active sports than other age or sex groups, leading to substantially more fractures.
INTRODUCTION
Many reports have described nasal bone fractures in adults, but there are few clinical reports of them in adolescents, although adolescence is the main growth period of the nasal bone. Previous studies have also tended to classify and describe child and adolescent nasal fractures in the same category [1,2]. However, there are significant differences in anatomy, parental care, social relationships, and social activities between children under the age of 12 and adolescents between the age of 13 to 18 [3,4]. In light of the emerging need as the need to classify adolescent nasal fractures separately, the present study was conducted to identify the clinical aspects of adolescent nasal fractures and aimed to establish the characteristics of nasal fractures in terms of the etiology and predominant patterns of prevalence compared to pediatric and adult populations.
METHODS
A retrospective review from March 2012 to February 2020 was conducted of the medical records of adolescent patients between the age of 13 to 18 who had isolated nasal bone fractures. This study excluded patients with other facial fractures, previous fracture history, surgical history, or congenital deformities. Information was extracted on patients’ demographic characteristics, such as sex, age, etiology, whether they underwent surgery, fracture type, the presence of a septal fracture, and whether there were any postoperative complications. Fracture evaluation was performed with a dual 128-channel CT scanner (SOMATOM Definition Flash; Siemens, Munich, Germany), and nasal bone fractures were classified using the system developed by Stranc and Robertson [5], as follows: plane I frontal impact (F I), plane II frontal impact (F II), plane I lateral impact (L I), plane II lateral impact (L II), and comminuted (C).
RESULTS
This study included a total of 269 patients (243 boys and 26 girls). Of these patients, 182 underwent closed reduction and 87 received conservative treatment, involving two who refused surgery (Table 1). According to the etiology, the number of patients was 85 for interpersonal violence, 79 for sports accidents, 40 for slip down injuries, 36 for bumping accidents, 16 for traffic accidents, 12 for accidents on motorcycles, and one for fall down injuries (Fig. 1). The number of frontal impact injuries was 128, that of lateral impact injuries was 132, and that of comminuted fractures was nine. Septal fractures were present in 97 patients, of whom 95 underwent had closed reduction and only two received conservative treatment (Table 1). The immediate postoperative results in anatomical restorations of the nasal skeleton without displacement or irregularity of fracture segments were analyzed in 143 patients. Good reduction with minimal displacement or irregularity was found in 120 cases after closed reduction. However, there were postoperative complications included three cases of deviated nose, two cases of saddle nose, and one case of hump nose.
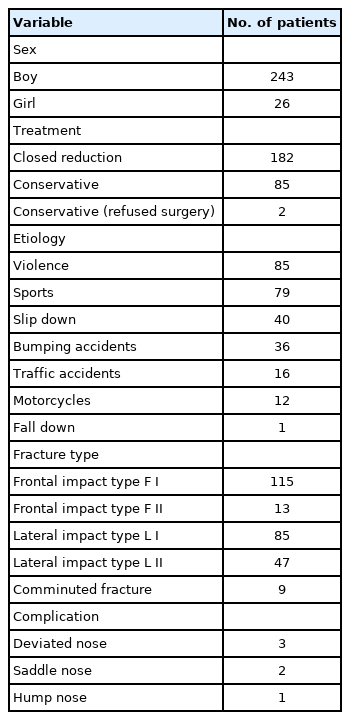
Patient demographics

The etiology of adolescent nasal fractures. The main causes of fractures were interpersonal violence and sports-related accidents, with numbers of 85 (31.60%) and 79 (29.37%), respectively.
DISCUSSION
In recent years, major concerns related to the management of pediatric nasal bone fractures have emerged, and some studies on this issue have been published. However, there are few studies on clinical aspects and characteristics of nasal bone fractures in adolescents, even though adolescence is the major growth period of the nose.
The first peak growth of the nasal bone takes place between the ages of 2 and 5, after which the nasal bone grows gradually. Major growth of the nasal bone occurs during puberty between the ages of 13 and 18, and additional growth of the septum occurs until the age of about 25 [6,7]. In addition, adolescents have significant differences from children and adults in anatomical characteristics, parental care, social relationship formation, and social activity. Therefore, as adolescent nasal fractures need to be classified separately, we investigated the clinical aspects and characteristics of adolescent nasal fractures. Most of the cases analyzed in this study were Korean adolescents, and this study showed that adolescent nasal bone fractures in Korean populations have several distinct characteristics in several points.
First, regarding the cause of nasal fractures, a study conducted in the United States and Canada found that there were many causes of acute falls in children and sports-related injuries in adolescents [8]. In Korea, it was reported that the predominant causes in the 12- to 14-year-old group were violence (38.33%) and sports (28.89%), and similar findings were observed in the 15- to 17-year-old group (32.92% for violence and 34.16% for sports); in contrast, fall or slip down injuries were the most common cause of fractures in patients younger than 12 years old [9]. In this study, as in previous studies, the main causes of fractures in adolescents between age 13 and 18 were interpersonal violence and sports-related accidents, and the numbers were 85 (31.60%) and 79 (29.37%), respectively. These results reveal that violence in the adolescent population is a serious social issue in Korea and that social activities including sports are common in adolescence [10].
Second, adolescent nasal fractures occurred more frequently in boys than in girls, with numbers of 243 (90.33%) and 26 (9.67%), respectively. There have been reports that the ratio of men to women across all age groups for nasal bone fractures is about 3:1 [11] or 4:1 [9] or 6:1 [12], but in this study, boys accounted for more than 90% of fractures in adolescents. The male predominance of nasal fractures in adolescents is believed to be due to differences in the diverse social and sports activities of boys compared to adolescent girls.
Third, it was reported that the lateral impact type was about twice as common as the frontal impact type in adolescents [9]. In this study, 115 patients had frontal impact type I fractures, 13 had F II fractures, 85 had L I fractures, 47 had L II fractures, and nine had comminuted fractures. There was no significant difference in the vectors of injury between frontal and lateral forces.
Fourth, the concomitant incidence of septal fractures in nasal bone fractures in all generations was reported to be 46.9% and 47.4% [12,13], and the frequency of septal deformities in Korea was reported to be about 18.1% in newborns [14]. Because a septal injury may cause deterioration of facial growth and deformity by disturbing a growth center—more specifically, the sphenodorsal and sphenospinal zones—the presence or absence of concomitant septal injuries in adolescent nasal bone fractures is a very important concern [15]. In this study, the overall number of septal fractures in adolescents with nasal bone fractures was 97 (36.06%). Furthermore, 95 patients (52.20%) among the 182 who underwent closed reduction showed septal fractures, whereas only two patients (2.30%) among the 87 who received conservative treatment showed septal fractures. These results indicate that patients with minor fractures seem to have few septal fractures (Table 2).
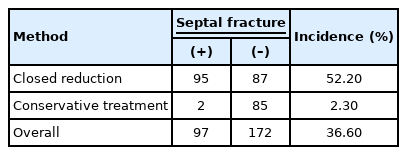
Incidence of septal fracture according to the method of treatment
Fifth, 182 patients underwent closed reduction under general anesthesia within 14 days of the initial injury, except eight cases in which the operation time was 15 days to 30 days because of late visits or improper conditions for the patient to undergo surgery.
The proportion of patients who underwent surgery was 67.66% in the adolescent group, while it was 23.47% in the pediatric group in the same study period; therefore, it was considered that the pattern of fractures in adolescents was more severe than that in children. The immediate postoperative results were evaluated through the comparison of preoperative and immediately postoperative computed tomography (CT) images. Accurate reduction without displacement or irregularity of fracture segments (Fig. 2) was achieved in 143 cases (78.57%), and good reduction with minimal displacement or irregularity was shown in 120 cases (44.61%). Poor results with deviated, saddle, or hump nose were shown in six cases, all of which had septal fractures.

Computed tomography (CT) image of a 16-year-old boy who sustained a nasal bone fracture after being hit by his friend’s elbow while playing basketball and underwent closed reduction. Preoperative CT image (A) shows a frontal impact injury (F II) with multiple, segmental fractures in the cephalic area and (B) with bilateral displacement of fracture segments into the nasal cavity in the caudal area, accompanied by a septal fracture. Postoperative CT image (C, D) shows an excellent result without any displacement or irregularity of fracture segments.
The 85 cases of conservative treatment, excluding two cases in which the parents refused surgery, had essentially no septal fractures. The criteria for conservative treatment were a linear fracture, a small fracture limited to a certain region, or the confined displacement of the fracture segment within the thickness of the nasal bone with a favorable nasal pyramid. The rest of the cases were treated by closed reduction. Among the 87 patients who received conservative treatment, three had follow-up CT examinations with agreement of the patients and their parents, and the examination time was 41 days, 40 days, and 3 years and 10 months (Fig. 3), respectively, after the initial injury. The follow-up results were favorable, without nasal skeletal asymmetry or irregularity. The other patients who received conservative treatment did not undergo follow-up CT examinations, and did not show any nasal deformity or discomfort at 1 month after the initial injury, and based on these results, favorable bone remodeling could be expected after long-term follow-up in minor adolescent nasal fractures, as in the pediatric nasal bone fracture [16].

Computed tomography (CT) image of an 18-year-old boy who sustained a nasal bone fracture after slipping down while going up the stairs and received conservative treatment. Initial CT image (A) shows a frontal impact injury (F I) with a linear fracture on the right nasal wall, a slightly displaced fracture on the left nasal wall, and a minor septal fracture. Follow-up CT image at 3 years and 10 months after the initial injury (B) shows excellent spontaneous bone remodeling with only conservative treatment; there was no nasal skeletal asymmetry or irregularity.
The major limitation of this study is a lack of long-term follow-up in both surgical and conservative treatment cases, and there needs to be further research on several parameters comparing adolescent nasal fractures to pediatric or adult fractures.
Notes
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Ethical approval
The study was approved by the Institutional Review Board of Daegu Catholic University Medical Center (IRB No. CR-21-170-L). The informed consent was waived.
Patient consent
The patients’ guardians provided written informed consent for the publication and the use of the patients’ images.
Author contribution
Conceptualization: Dong Gil Han, Sung-Eun Kim, Yong Jig Lee, Jeong Su Shim. Data curation: Se Hun Kim. Formal analysis: Se Hun Kim, Dong Gil Han. Methodology: Sung-Eun Kim, Yong Jig Lee, Jeong Su Shim. Investigation: Se Hun Kim, SungEun Kim, Yong Jig Lee. Resources: Dong Gil Han. Supervision: Dong Gil Han, Jeong Su Shim. Writing - original draft: Dong Gil Han. Writing - review & editing: Se Hun Kim, Sung-Eun Kim, Yong Jig Lee, Jeong Su Shim.
Abbreviations
CT
computed tomography
F I
plane I frontal impact
F II
plane II frontal impact
L I
plane I lateral impact
L II
plane II lateral impact
C
comminuted