INTRODUCTION
Xanthelasma palpebrarum (XP) is a benign periorbital tumor. The term xanthelasma was first proposed by the 19th-century English surgeon and dermatologist, Sir Erasmus Wilson, derived from the Greek words âXanthosâ (yellow) and âElasmaâ (beaten metal plate) [1]. As the name suggests, XP presents as yellowish papules or plaques on the eyelids.
The prevalence of XP is approximately 1.1% in women and 0.3% in men [2]. XP is known to be associated with hypercholesterolemia, and reports indicate that approximately 50% of patients diagnosed with XP also have hypercholesterolemia [2]. Histologically, xanthelasmas are composed of foam cells, which are lipid-laden histiocytes [3]. These foam cells accumulated mainly in the upper reticular dermis layer near the capillaries, appearing as yellowish skin lesions. Considering the pathogenesis, leakage of low-density lipoprotein (LDL) from the capillaries is an important aspect of the disease etiology [3,4]; mechanical movement and friction, heat, and inflammatory responses accelerate the leakage of LDL. These factors are prevalent around the eyelids, explaining the higher incidence of xanthelasma appearance compared other parts of the body [5].
Many studies have studied the clinical characteristics of xanthelasma, however, few studies have investigated the size of XP and the relationship between other clinical features. Therefore, in this study, we analyzed the size of XP lesions and their clinical characteristics to examine the relationship between elevated serum cholesterol levels and XP size.
METHODS
Study design and patients
We conducted a retrospective chart review of patients diagnosed with XP, who underwent surgery between August 2014 and September 2021. The participants of this study were patients with suspected XP lesions, confirmed by biopsy, in whom serum cholesterol levels were measured preoperatively. A total of 41 patients were clinically suspected of XP and underwent surgery. Four patients were excluded from the analysis because the pathologic diagnosis was not made. Three of the remaining 37 patients were excluded from the study because their serum cholesterol levels were not measured. A total of 34 patients were included in the analysis.
Evaluation of outcomes
We investigated the patientâs lesion size and location, serum total cholesterol level, underlying disease, and XP recurrence. Serum cholesterol levels were divided into normal (<200 mg/dL), intermediate (200â239 mg/dL), and hypercholesterolemia (âĽ240 mg/dL) groups. The area of the xanthelasma was assumed to have an elliptical shape and was calculated using the long (a) and short axis (b) measured preoperatively. If there were multiple lesions, the size of each lesion was added (Fig. 1).
The lesions were classified according to the grading system proposed by Lee et al. in 2013 [6]. Lesions of grade I were limited to the upper eyelid, grade II involved the medial canthus, grade III affected both eyelids on the medial side, and grade IV involved both medial and lateral sides of the upper and lower eyelids (Fig. 2).
Operative technique
All patients underwent xanthelasma excision under local anesthesia. A simple excision of the lesion in an elliptical shape was generally performed to prevent eyelid deformities. In cases with multiple lesions, each lesion was excised through a different incision (Fig. 3). If the lesion had a diffuse distribution, a local flap or upper blepharoplasty was performed to prevent eyelid deformity (Fig. 4). Invasion of the xanthelasma into the orbicularis oculi prompted excision of the affected muscle section. The skin was repaired using black silk 7-0 sutures.
Statistical analysis
Continuous variables between groups were compared using Mann-Whitney U and Kruskal-Wallis tests. In addition, the one-sample Wilcoxon signed-rank test was used to compare the patientsâ average serum cholesterol levels with those of the general population. Statistical significance was set at p<0.05. All analyses were performed using IBM SPSS Statistics for Windows (version 25.0; IBM Corp., Armonk, NY, USA).
RESULTS
Of the 34 patients analyzed, 12 were men (35.3%) and 22 were women (64.7%). The patientsâ age at the time of surgery ranged from 34 to 74 years, with a mean age of 53.0 years. Grade I lesions were the most common (52.9%), followed by grades III (17.6%), II (14.7%), and IV (14.7%). Regarding the laterality of the lesion, 10 patients (29.4%) showed unilateral lesions and 24 patients (70.6%) showed bilateral lesions (Table 1).
The mean serum cholesterol level in all patients was 235.0 mg/dL. When the XP patients were classified by sex, serum cholesterol level was found to be 234.8 mg/dL in men and 235.2 mg/dL in women. As reported by a paper published in 2021 [7], the average cholesterol level in Korean adults was 192 mg/dL in men and 194 mg/dL in women. In this study, the serum cholesterol level was found to be higher in both men and women compared to the Korean general population (p=0.003 and p<0.001) (Fig. 5).
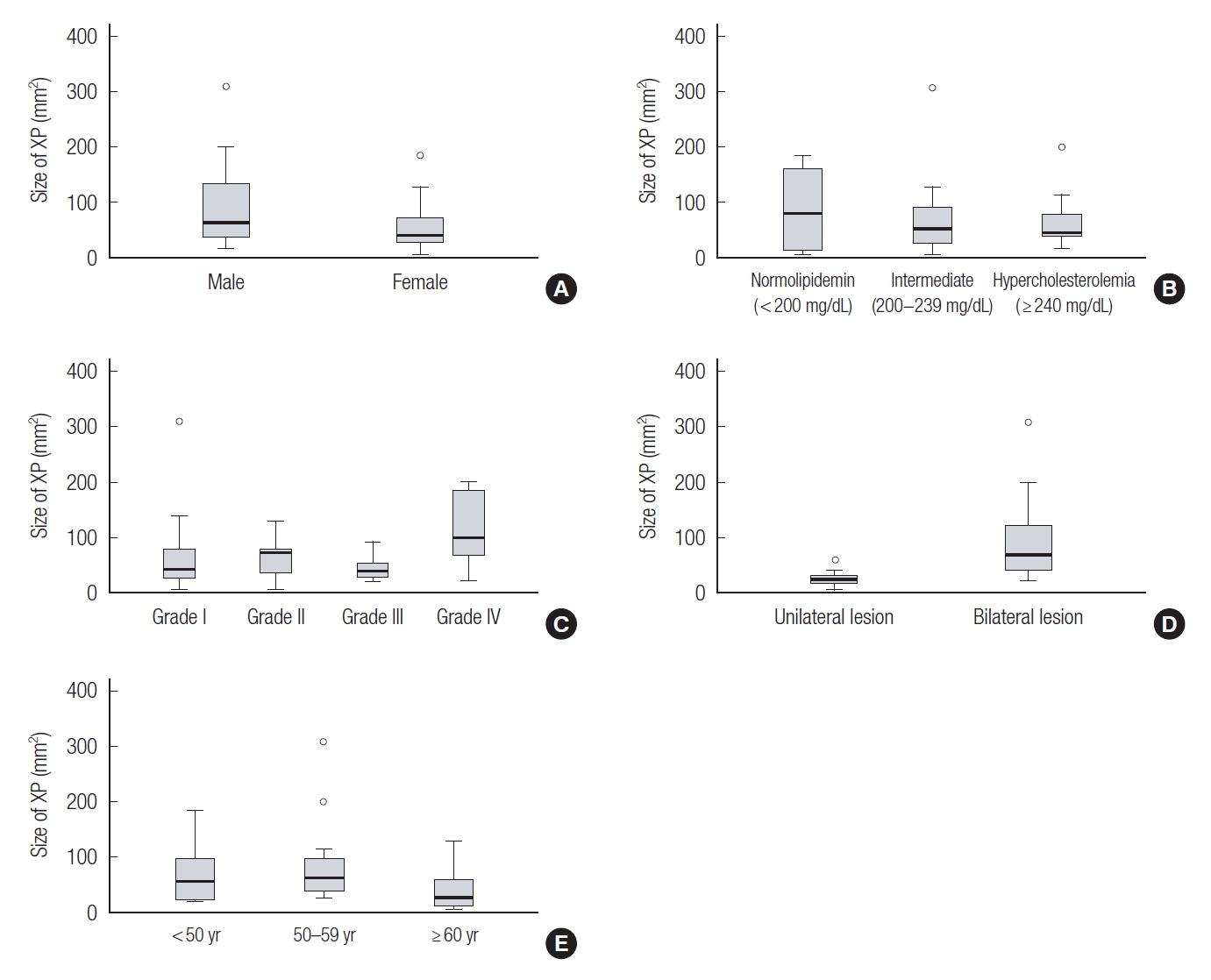
XP size was compared according to sex, grade, laterality, and serum cholesterol levels. The mean lesion was 69.2 mm2. According to the serum cholesterol level, the normal cholesterol group was largest size (87.0 mm2), followed by the intermediate group (69.8 mm2) and hypercholesterolemia group (63.1 mm2). However, the difference was not statistically significant. In addition, there were no significant differences in xanthelasma grade, age, or sex. The only significant difference was found in laterality, where bilateral lesions (87.8 mm2) were larger than unilateral lesions (24.7 mm2) (Table 2, Fig. 6).
DISCUSSION
This was a retrospective study investigating the relationship between XP size and other clinical characteristics. As in previous studies, XP was prevalent in middle-aged women [2,8]. In addition, grade I lesions involving only the upper eyelid were the most common, with the lesions coinciding on both sides. In this study, surgical excision was performed in all xanthelasma patients. Since the eyelids are the important structure that protects and lubricates the globes and cornea, it is essential to preserve their structure [9,10]. In most cases, simple excision followed by primary closure was enough. However, if the lesion had diffuse distribution, we performed local flap techniques or upper blepharoplasty in order to avoid eyelid deformity [4,6,11].
In papers published in Western countries, approximately 50% of patients with XP are associated with hypercholesterolemia [2]. Similarly, in a study conducted in Taiwan, dyslipidemia was present in 50% of patients [8]. This study found that approximately 38.2% of patients had hypercholesterolemia in the preoperative evaluation. This result is estimated to be higher than the prevalence of 20.7% in the general population of Korea [7].
Although there was no statistically significant difference in the size analysis of patients with XP, several trends could be identified. Most patients with XP ranged from 50 to 59 years of age, and the lesion size was the most extensive among these patients. XP is a more prevalent disease in women, but paradoxically, its size tends to be larger in men. It could be explained that women are more sensitive to facial aesthetics than men, so they are apt to come to the hospital for surgery.
A limitation to the generalizability of this study is that the sample size is relatively small and that it was conducted only at a single center. Therefore, a further large-scale study is needed. Another limitation was that other lipid profiles, including LDL cholesterol, were not examined. Meanwhile, in this study, comparing the serum cholesterol level with the general population requires careful interpretation. Since the analysis was performed on patients who underwent surgical treatment at the plastic surgery department, the possibility of selection bias should be considered. Also, in the case of patients taking lipidlowering medications, serum cholesterol may be lowered by the drug, so it is necessary to analyze them separately to account for this discrepancy. However, this study is limited in that it could not be implemented due to the omission of records, possibly leading to confounding bias.
This study compared lesion size with various clinical features in XP patients. In patients who underwent surgery for XP, blood cholesterol levels tended to be higher than those in the general population. However, the trend between the size of XP and serum cholesterol level was unclear. Therefore, if a patient with XP visits the hospital for surgery, it is recommended to check the lipid profile to confirm underlying dyslipidemia regardless of the size.