A vertically split fracture of the marginal tubercle of the zygoma in a 3-year-old boy: a case report
Article information

Abstract
Fractures of the zygoma are rarely encountered in pediatric patients. This report presents a case of a 3-year-old child who presented with a vertically split fracture of the marginal tubercle of the zygoma. The marginal tubercle, a bony portion present on the posterior border of the frontal process, assists in attaching the temporalis fascia. This patient was treated surgically with bony fixation using tissue glue. To the best of our knowledge, no cases of fracture of the marginal tubercle of the zygoma have been reported in the literature. Fractures of the marginal tubercle of the zygoma in pediatric patients may be overlooked because of their anatomic location and the musculoskeletal characteristics of these patients. Here, we discuss the clinical features of marginal tubercle fractures of the zygoma.
INTRODUCTION
The pattern of facial fractures differs between pediatric and adult patients. Children who are younger than 5 years account for only 0.9% to 1.2% of cases of facial fractures overall and 20.2% of cases of facial fractures in pediatric patients [1,2]. Midfacial fractures are uncommon in pediatric patients because of their skeletal elasticity, lack of sinus pneumatization, thicker bones, and high cranium-to-face ratio [3].
The zygoma has a quadrangular shape and possesses the frontal, temporal, maxillary, and orbital processes. The tubercle that projects posteriorly from the frontal process is called the marginal tubercle. The marginal tubercle of the zygoma serves as an attachment site for the fascia of the temporalis muscle, and the temporalis muscle acts as the primary mover of the mandible in mastication [4]. Here we present an unusual pattern of zygomatic fracture in a 3-year-old child in which the marginal tubercle was split vertically.
CASE REPORT
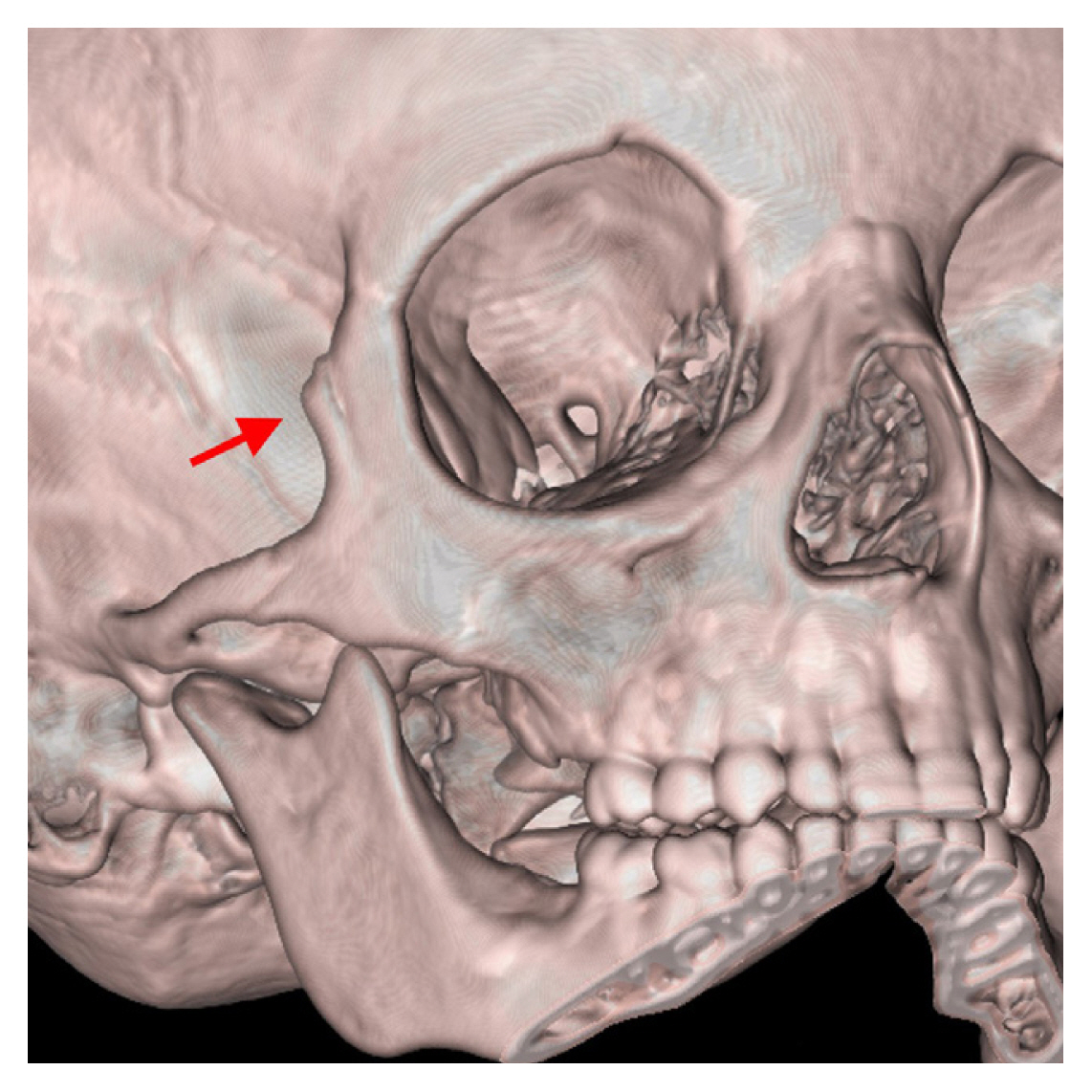
A 3-year-old child visited our department after falling from a motorbike and hitting his head against the ground. When he tried to open his mouth, severe pain developed in the lateral orbital area and restricted mouth opening was observed. There was no facial palsy. A step deformity was palpated in the lateral orbital area. Three-dimensional computed tomography revealed a vertically split fracture of the marginal tubercle of the zygoma (Fig. 1). An open wound was observed on the right side of the preauricular area, but no external wound was noted on the fracture site (Fig. 2). Closed reduction failed to stabilize the fragment. One week after the injury, the pain in the lateral orbital area during restricted mouth opening persisted. Therefore, open reduction was planned. A small incision was made, and an outwardly displaced segment of the marginal tubercle was noted (Fig. 3). The fractured segment was reduced. For bony fixation, we used tissue glue, N-2-butyl cyanoacrylate (enbucrilate; Histoacryl, B. Braun Melsungen AG, Tuttlingen, Germany). A computed tomography scan taken 7 days postoperatively showed that the reduced marginal tubercle alignment was maintained (Fig. 4). Moreover, the palpable step deformity and restricted mouth opening had resolved completely and no facial palsy was noted.
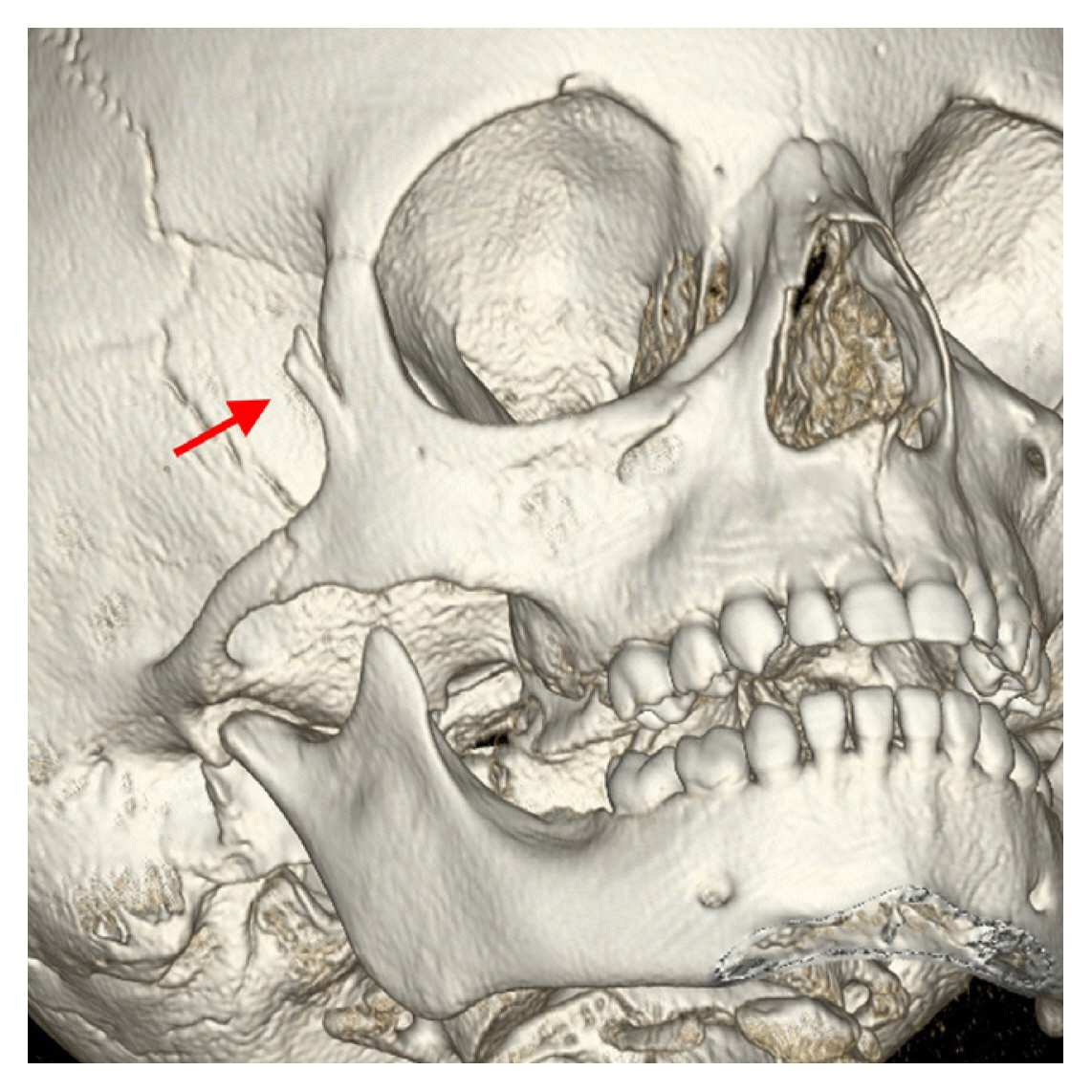
Preoperative computed tomography showing a vertically split fracture of the marginal tubercle of the zygoma (red arrow).

Preoperative photograph of the open wound in the zygomatic arch. Note the lack of an external wound in the lateral canthal area.

Intraoperative photograph of a small incision made to repair the fractured area, exposing the displaced segment of the marginal tubercle. The outwardly displaced segment of the marginal tubercle is visible.
Postoperative computed tomography showing reduction of the fractured segment to its appropriate position (red arrow).
DISCUSSION
The frontal process of the zygoma possesses a posterior projective edge called the marginal tubercle. The temporalis fascia inserts into the marginal tubercle of the zygoma; occasionally, the temporalis muscle itself is directly attached (Fig. 5) [5]. From an anatomical point of view, it is assumed that a vertically developing split fracture along the marginal tubercle can occur depending on the direction in which the temporalis fascia and temporalis muscle are attached. In children, the skeleton has a higher cranium-to-face ratio and thicker overlying soft tissue and fat [6]. Because no external wound to the skin was noted at the fracture site, we presumed that the trauma force was not delivered directly to the fracture site; rather, the force was delivered to the temporal fossa and transmitted to the marginal tubercle through the temporalis fascia and temporalis muscle. That is, the patient’s fracture was considered to have been caused by an indirect rather than direct force.

Anatomical relationships of the temporalis fascia (blue color) and temporalis muscle (red color) inserting into the marginal tubercle.
We hypothesized that the bulkiness of the temporalis muscle allowed the fracture of the marginal tubercle to occur in an out-fracture rather than in an in-fracture fashion. Ranganathan et al. [7] reported an inverse correlation between age and temporalis muscle thickness. The pediatric skeleton also has higher elasticity and a higher cancellous to cortical bone proportion [6]. Increased skeletal flexibility results in more malleable bone stock and greater suture compliance. For these reasons, we postulate that an incomplete (greenstick) fracture is more likely to occur than other types of fractures, as in this case.
We attempted closed reduction, but the fractured segment was not stabilized; thus, we believed that bony fixation through open reduction would be necessary. Especially in children, rigid fixation carries a risk of restriction or delayed growth [8]. It is also possible that extrusion, migration, and pain from palpable hardware may occur. Moreover, bony fixation with miniplates and screws is difficult to perform and carries the possibility of significant bone tissue loss if the bony fragment is very thin and small. Accordingly, we decided to use N-2-butyl cyanoacrylate in this case [9–13]. We believed that fixation using the N-2-butyl cyanoacrylate glue provided sufficient stability because the fracture was incomplete (greenstick) and not in an area to which great force or pressure was delivered. Compared to fixation using hardware, the postoperative cost was low and the cosmetic results were excellent.
Several studies have presented unusual patterns of midfacial fractures. Mermod et al. [14] reported a rare case of isolated bilateral zygomatic fractures in a 32-year-old man. In the pediatric population, nasal bone fractures are common [15], while isolated zygomatic arch, alveolar ridge, maxillary sagittal, and LeFort fractures are unusual [16]. However, to the best of our knowledge, there are no published cases with the pattern of zygomatic fracture described here.
Pediatric facial fractures differ from adult facial fractures. Therefore, in the treatment of fractures in children, fractures due to indirect forces are possible, leading to the need to be aware of the possibility of injuries in areas other than the visible wound. Thus, fixation using tissue glue may be a good alternative in areas that are not under significant force.
Notes
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Ethical approval
The report was approved by the Institutional Review Board of Soonchunhyang University Hospital (IRB No. 2022-08-006).
Patient consent
The patient’s parents provided written informed consent for the publication and use of his images.
Author contributions
Conceptualization: Chul Han Kim. Data curation: Chan Yeong Lee. Formal analysis: Chan Yeong Lee. Funding acquisition: Chul Han Kim. Methodology: Chul Han Kim. Project administration: Chul Han Kim. Visualization: Chan Yeong Lee. Writing - original draft: Chan Yeong Lee. Writing - review & editing: Chul Han Kim. Approval of final manuscript: all authors.