Unusual anomaly of the radial artery encountered during the elevation of a radial forearm free flap: a case report
Article information

Abstract
The radial forearm free flap (RFFF) has become popular for head and neck reconstructions. Owing to a constant anatomy the RFFF is relatively easy to dissect. Nevertheless, anatomical variations of the radial artery have been reported. Some variations could affect the survival of the flap. This paper reports an unusual anomaly of the radial artery where the radial artery was not located between the brachioradialis (BR) and flexor carpi radialis. The radial artery was observed above the BR and on the radial side of the BR. The survival of the elevated flap was deemed questionable because it had only few perforators. So we decided to discard the flap and to elevate another free flap for the head and neck defect. The donor area on the forearm was covered using the original skin of the first flap as a full-thickness skin graft. This case highlights a means to deal with anomalies of the radial artery encountered during the elevation of RFFF and the checking process for variations of the radial artery before RFFF.
INTRODUCTION
The radial forearm free flap (RFFF) is used widely to reconstruct the head and neck area. This flap is thin and has excellent pliability, ease of flap elevation, and a long pedicle length [1,2]. The radial artery originates from the brachial artery, where it bifurcates in the cubital fossa. The radial artery is in the intermuscular septum between the brachioradialis (BR) and flexor carpi radialis (FCR). It forms the deep palmar arch of the hand with the deep palmar branch of the ulnar artery. The modified Allen’s test can help to test the continuity of the palmar arch and determine if there is any potential radial-sided vascular insufficiency resulting from the loss of continuity of the radial artery. Although there is consistency in the anatomy of the radial artery, there are some reports on anomalies and variations of the radial artery. This paper reports the case of a patient with a variation of the distal radial artery observed during flap elevation despite having displayed a normal modified Allen’s test.
CASE REPORT
A 58-year-old man presented with an ulcerative mass on the right buccal mucosa and retromolar trigone. He was a past smoker with 20 pack-years and quit smoking for the last 15 years earlier. He also had diabetes and Bechet’s disease. The mass was diagnosed as a squamous cell carcinoma through a histological examination. Imaging studies were performed, and the TNM stage was T3N3M0. After a wide excision via the trans-oral approach with a modified radical neck dissection by the otorhinolaryngology team, the final defect size was 5.0×4.5 cm, and the required pedicle length was 5 cm. Reconstruction with a fasciocutaneous RFFF was planned to cover the defect. The modified Allen’s test showed normal blood flow through the radial and ulnar arteries. A 250-mmHg tourniquet was applied before the dissection. The anatomic landmarks of the RFFF, the palmaris longus, FCR, and BR were marked. The design of the skin paddle (6.5×5.5 cm) was also marked on the left forearm (Fig. 1A). After tourniquet inflation the flap was elevated from the flexor carpi ulnaris muscle to the FCR on the suprafascial level starting at the ulnar side. On the radial side, the fascia of the BR was dissected. Unexpectedly, the radial artery was absent between the BR and FCR (Fig. 1B). Instead, the radial artery course was above the surface of the BR near the distal third of the forearm and ran with the cephalic vein on the radial side of the BR. In the distal area of the radius, there was a large aberrant branch of the cephalic vein between the BR and FCR (Fig 1C). It was difficult to have proper perforators in the elevated flap because of the deviation of the radial artery. Therefore, the plan was changed from an RFFF to an anterolateral thigh free flap. With the elevated radial forearm flap, a full-thickness skin graft was performed on the same donor (Fig. 1D). The defect was reconstructed successfully with an anterolateral thigh free flap. There were no major complications on the distal forearm after the full-thickness skin graft (Fig. 2).
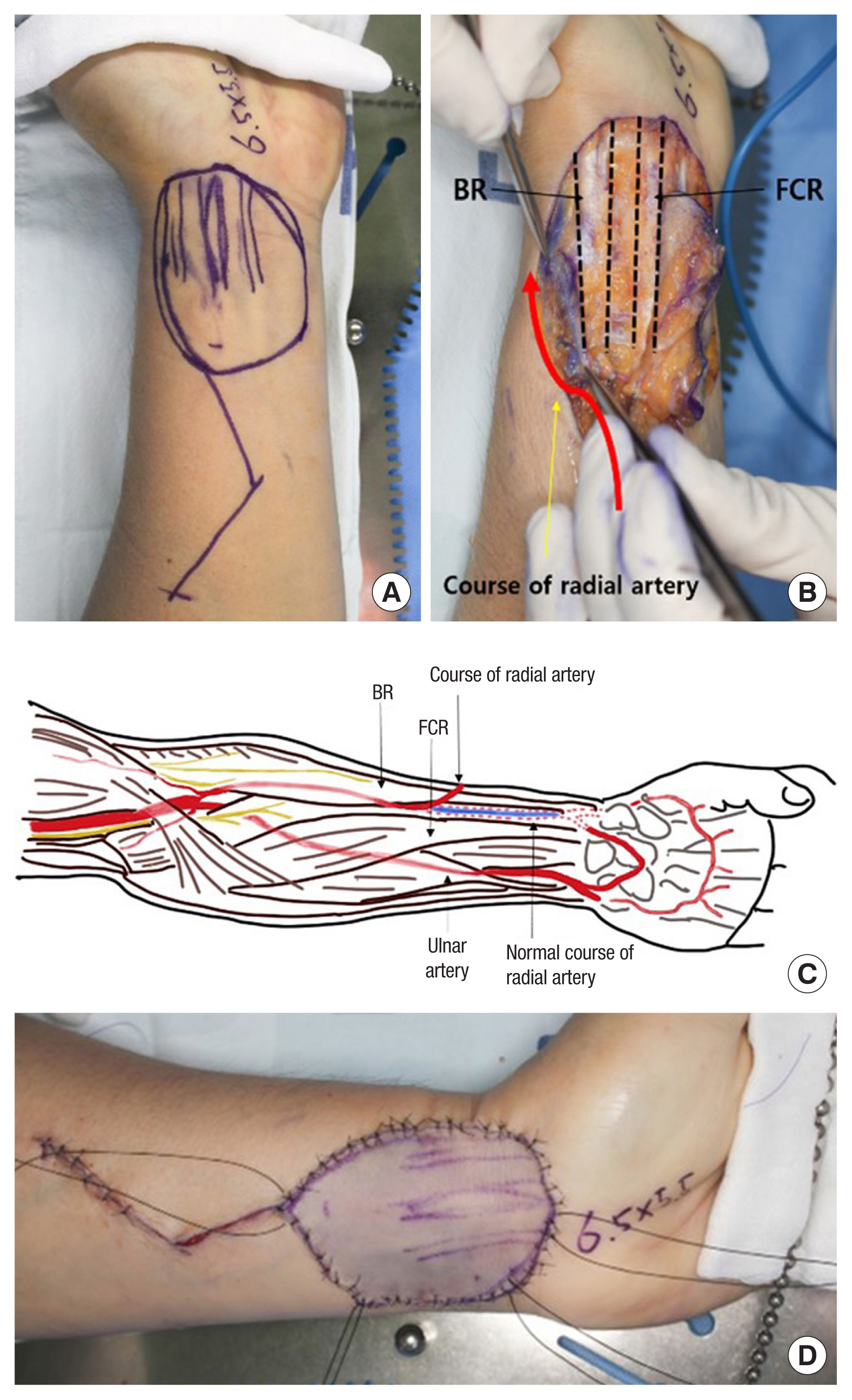
Intraoperative photographs. (A) Flap design of the radial forearm free flap. (B) The variation of the radial artery was seen. The radial artery ran with the cephalic vein on the radial side of the BR. The aberrant branch of the cephalic vein ran between BR and FCR. (C) Schematic diagram, palmar view. (D) Full-thickness skin graft from the elevated radial forearm flap. BR, brachioradialis; FCR, flexor carpi radialis.

Postoperative photographs at 2 months.
DISCUSSION
The radial artery is usually bifurcated from the brachial artery approximately 1 cm distal to the antecubital fossa. In the distal third of the forearm, the radial artery becomes superficial in the anterior of the radius and lies between the tendons of the BR and FCR.
The constant anatomy of the radial artery makes it very useful for RFFF, radial artery access for coronary artery intervention, and radial artery puncture. On the other hand, there are some reports of anatomic variations. McCormack found with a cadaver study that the incidence of anatomical variations of the radial artery was 4.3% of the 750 extremities examined [3]. Uglietta and Kadir [4] reported 9% of anomalies of the radial artery out of 100 upper extremity angiograms. Hoffman et al. [5] performed a meta-analysis to estimate the prevalence of anatomical variations in the radial arteries. Their meta-analysis showed that anatomical variations in radial arteries occurred in 10.5% of patients. These anatomical variations included an abnormal origin (5.6%), tortuous configuration (4.3%), hypoplasia (1.9%), stenosis (1.3%), radial artery loops (0.9%), and radial artery accessory branches (0.5%). The tortuous configuration and radial loops can make pedicle dissection difficult. Accessory branches of the radial artery are rare but are usually found intra-operatively and carry the risk of affecting flap harvesting and survival.
The preoperative modified Allen’s test revealed normal findings. The radial artery patency appeared normal because the radial artery ran along the radial side of the BR and dorsally at the 1/3 distal wrist (Fig. 3). After surgery, the mistake from the preoperative evaluation was found. The 3-dimensional (3D) angiograph was reviewed carefully, and the aberrant artery variation was identified. Indeed, finding the variation in 3D angiography was very difficult.
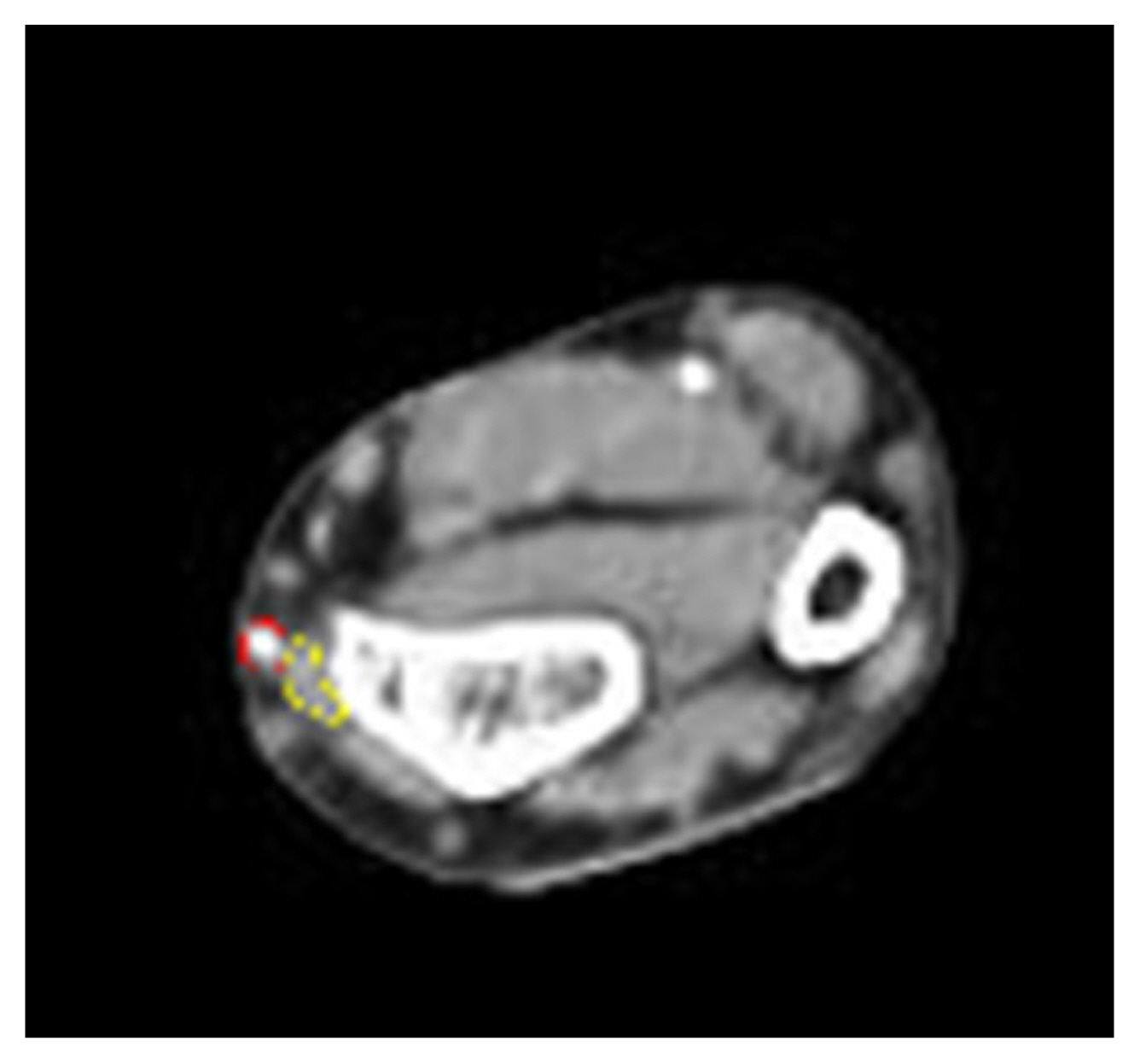
Preoperative 3-dimensional angiography of the upper extremities. The radial artery runs more along the radial side of the brachioradialis, not between the brachioradialis and flexor carpi radialis (red dot line: radial artery, yellow dot line: brachioradialis).
It is essential to ensure the anatomy and vascular condition of the donor site and exclude variations before surgery, but rare anomalies could occur. Although the preoperative modified Allen’s test and palpitation could detect an abnormal radial artery [6], preoperative ultrasonography also helps find radial artery anomalies unsuitable for RFFF with a high risk of flap failure [6,7]. Inappropriate detection and management of radial artery anomalies may result in a compromised surgical outcome because these anomalies of the radial artery could jeopardize the elevation of the RFFF [8,9]. If radial artery variations are encountered during surgery, it may be necessary to confirm whether the flap circulation is suitable through abnormal or aberrant vessel clamping [8].
This paper reports the authors’ experience of this rare case presenting with a radial artery variation in the distal forearm. In addition to the preoperative modified Allen test, plastic surgeons should be well-acquainted with 3D angiography and ultrasonography imaging if necessary. Careful dissection and ascertaining the course of the radial artery intraoperatively are essential for safe RFFF elevations.
Notes
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Funding
None.
Ethical approval
The study was approved by the Institutional Review Board of Inha University Hospital (IRB No. 2022-07-005).
Patient consent
The patient provided written informed consent for the publication and use of the images.
Author contributions
Writing - original draft: Jin Myung Yoon, Tae Jun Park. Writing - review & editing: Sae Hwi Ki. Resources: Jin Myung Yoon, Tae Jun Park. Supervision: Sae Hwi Ki, Min Ki Hong.
Abbreviation
3D
3-dimensional
BR
brachioradialis
FCR
flexor carpi radialis
RFFF
radial forearm free flap