INTRODUCTION
Fibrous dysplasia (FD) is a localized bone disorder that replaces normal bone structure with fibro-osseous tissue. FD accounts for approximately 6% of benign bone tumors, and patients affected in the craniofacial region often experience gradual swelling, deformity, and compromised vision or hearing [1ŌĆō3]. While the natural disease course can vary between patients, there exist three phases of FD progression: initial, growth or proliferation, and stabilization [4,5].
Surgery was previously indicated for FD lesions in the active growth phase that caused neurological, functional, or aesthetic concerns due to its invasiveness [3]. The two main surgical treatments are radical excision with reconstruction and conservative bone shaving. While radical excision is less prone to regrowth, it is invasive, has high expected blood loss, and has a longer healing time [6ŌĆō8]. On the other hand, conservative bone shaving provides relatively short-lasting results requiring reoperation every 2 to 4 years after surgery, and sometimes aesthetic concerns resurface after only a few months [9].
We previously introduced ŌĆ£the core extirpation method,ŌĆØ a novel surgical technique that is minimally invasive like traditional bone shaving but has longer-lasting effects [10]. Physical evaluations during clinical follow-up visits after the core extirpation technique in the zygomaticomaxillary region revealed no visible external regrowth during several years of monitoring. However, on computed tomography (CT) scans, refilling of the maxillary sinus by the remnant FD lesion was evident. This study presents the long-term outcomes of the core extirpation technique in managing zygomaticomaxillary FD.
METHODS
We retrospectively analyzed patients who underwent core extirpation for FD of the zygomaticomaxillary region between 2012 and 2021 at Seoul National University Bundang Hospital. This study was approved by the Ethics Committee of Seoul National University Bundang Hospital (IRB No. B-2104-676-103). Patient demographics, including age, sex, laterality, location, and initial symptoms, were compared. In this retrospective analysis, CT scans from each patient were analyzed chronologically.
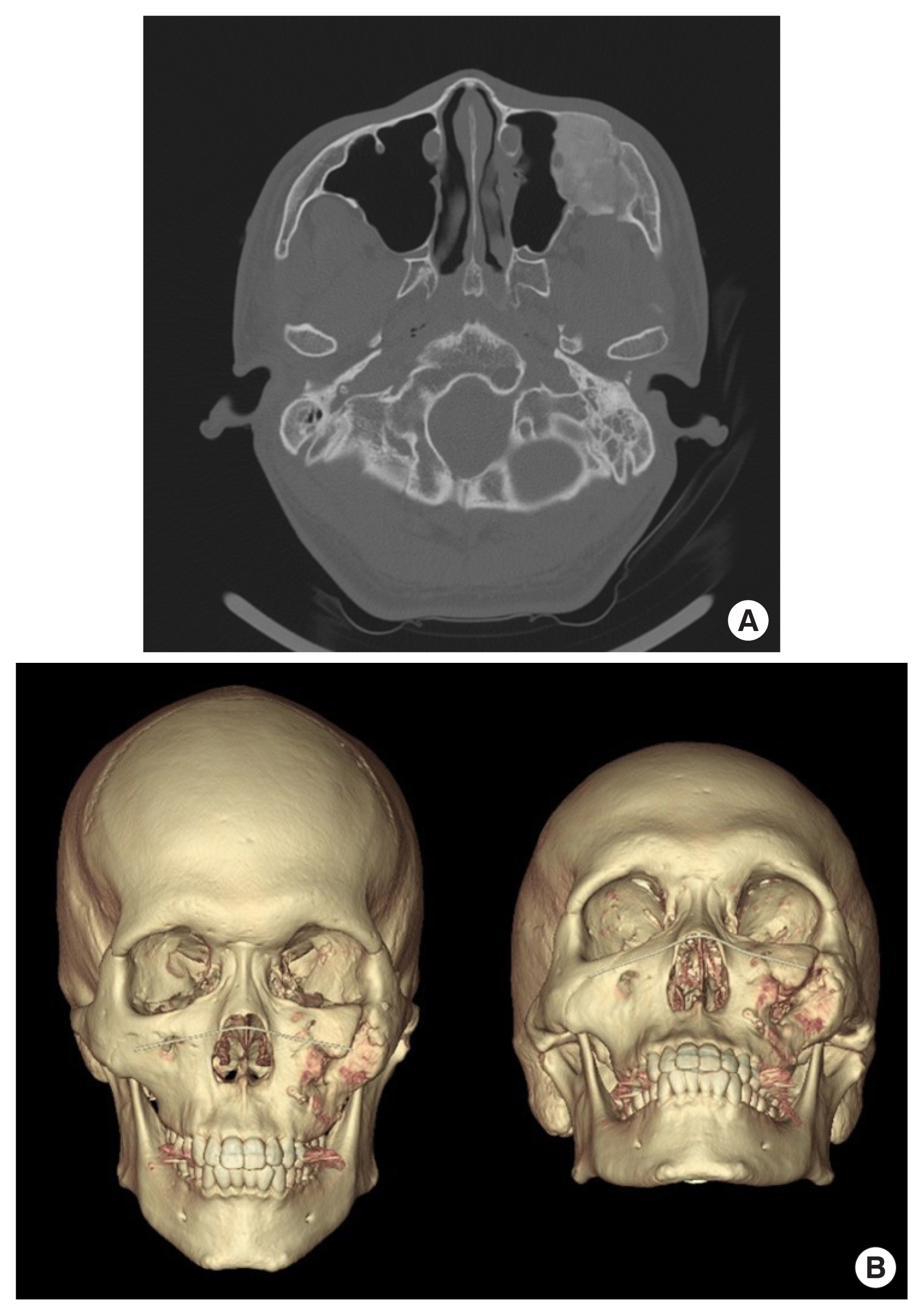
CT scans taken 6 to 12 months prior to the operation, immediately before and after the operation, and during follow-up visits were analyzed. Axial scans were used to measure the most prominent points of the zygomatic bone and to assess the discrepancies between the anteroposterior (AP) and mediolateral (ML) lengths between the affected and the unaffected sides (Fig. 1). Additionally, the volume of the FD lesion was manually measured from the axial cuts obtained in each scan.
All operations were performed under general anesthesia with the patient in the supine position and the head elevated. The upper gingivobuccal approach was utilized for subperiosteal dissection of the affected region to expose the lesion. A port in the anterior maxillary wall was created with a sagittal saw based on the preoperative CT scan, allowing access to the core of the lesion. The core of the lesion was extirpated while preserving the cortical structures of the zygoma and the maxilla to maintain symmetrical facial contour and improve aesthetic outcomes. Following core extirpation, the anterior maxillary wall and the zygomaticomaxillary complex were fixed using a miniplate if necessary to restore the buttresses. Further details of the core extirpation technique can be found in our previously published work [10].
RESULTS
A total of 12 patients (seven females and five males) were analyzed in this study. The mean age of the patients was 23.7 years (range, 11ŌĆō40 years). Ten Patients presented with painless swelling of the facial area, and FD was incidentally diagnosed in two patients during a CT scan. Five patients were affected on the right side, while seven were on the left. Follow-up periods ranged from 12 to 48 months, with a mean follow-up time of 28.8 months (Table 1).
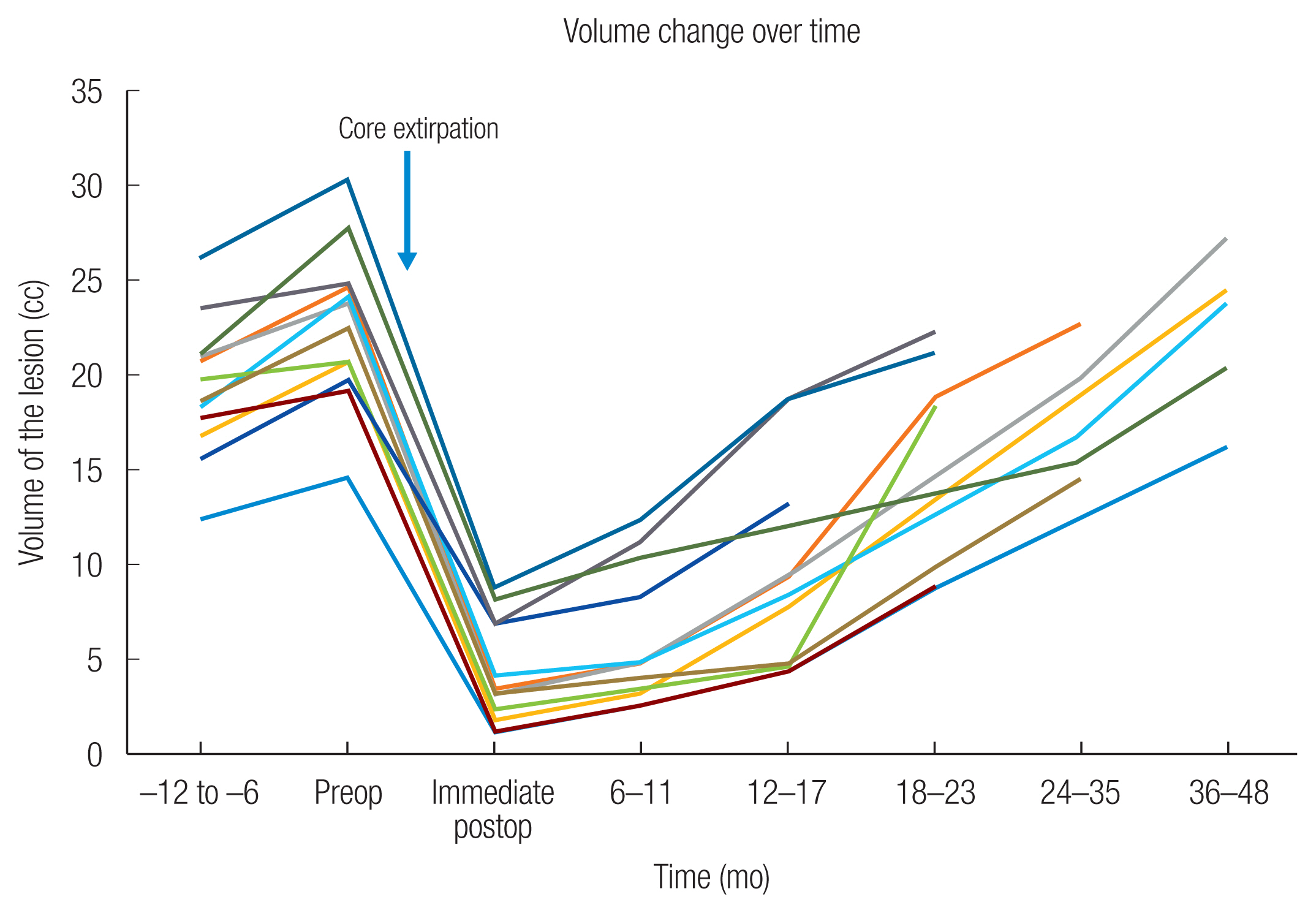
Chronological changes in the AP/ML discrepancies and the lesion volumes are summarized in Table 2 and Fig. 2. All 12 patients exhibited an increase in AP/ML discrepancies and volume from 6 to 12 months before the operation and immediate postoperative CT, indicating that all lesions were in the growth phase. The immediate postoperative AP/ML discrepancies were stable up to 12ŌĆō17 months postoperative in all patients. One out of seven patients with postoperative 18ŌĆō23 months CT scans (patient 3) had a slightly increased ML discrepancy from ŌłÆ1.1 to ŌłÆ0.5 mm, while the discrepancies were stable in the rest of the patients. In five patients with postoperative 24 to 35 months CT scans, the same patient (patient 3) showed increased ML discrepancy, while the other four had stable discrepancies. In four out of five patients with postoperative 36 to 48 months CT scans, AP/ML discrepancies increased. At 36 to 48 months, the median increase from immediate postoperative measurements was 0.78 mm in AP (range, 0ŌĆō2.7 mm) and 2.26 mm in ML (range, 0.1ŌĆō8.7 mm). Postoperative volumes showed continuous growth of the lesion, with a median volume growth rate was 0.61 cc per month (range, 0.33ŌĆō0.89 cc). The total volume exceeded preoperative volume in three out of five patients with postoperative 36 to 48 months follow-up CT scans.
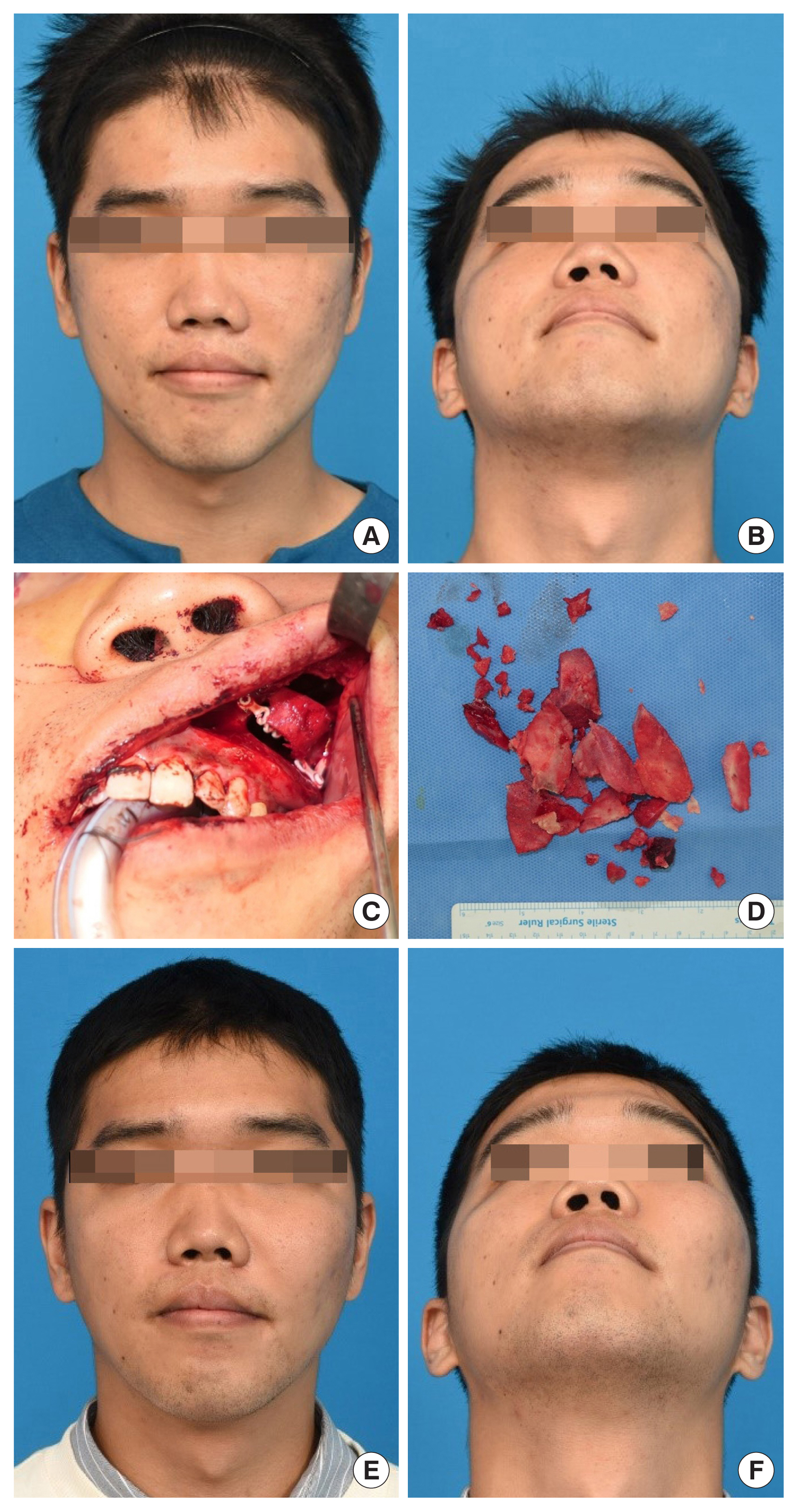
Representative case
A 28-year-old man presented with a painless slowly-progressing swelling of the left cheek (Fig. 3). He had no signs of vertical dystopia, exophthalmos, or optic nerve compression. A CT scan demonstrated FD of the left zygomaticomaxillary complex, with preoperative AP and ML discrepancies of 8.39 mm and 6.5 mm, respectively. The patient underwent core extirpation with zygoma reduction without any postoperative complications. Although postoperative CT scans at 12 months showed intralesional growth, there was no further external increase in the lesion nor any evidence of recurrence (Fig. 4).
DISCUSSION
FD of the zygomaticomaxillary complex lesion can result in facial asymmetry due to bulging. Available surgical treatments for this condition include radical excision with immediate reconstruction and shaving [11]. Despite the relatively short effectiveness of bone shaving, many surgeons resort to bone shaving due to the difficulty and invasiveness of complete wide resection, which often requires complex reconstruction [12,13]. Several studies have reported excellent cosmetic outcomes with bone shaving [14,15], although the long-term efficacy of this technique remains controversial [16,17].
To achieve longer-lasting effects while minimizing invasiveness, we employed the core extirpation method. This minimally invasive technique is associated with low expected blood loss and can be performed as day surgery, providing similar cosmetic outcomes as traditional bone shaving but with longer-lasting results. Our results demonstrated that AP/ML dimensions were stable up to 24ŌĆō35 months in all patients and that even after 36ŌĆō48 months, the changes in AP/ML dimensions were minimal (average of 2.26 mm) and often went unnoticed by the patients.
The pattern of regrowth following the initial operation may account for the longer-lasting effect of the core extirpation compared to bone shaving. In the case of traditional bone shaving, the regrowth of the lesion occurs outward, resulting in external changes that can manifest within a few months. In contrast, following core extirpation, the remnant lesion regrows within the hollowed-out (extirpated) core area, with outward regrowth occurring only after complete filling of the core.
Radical excision followed by immediate reconstruction is a viable treatment option to eradicate FD lesions and prevent recurrences. This approach is recommended for patients with fast-growing lesions causing neurological or optical symptoms. However, in patients without these symptoms, the core extirpation method can be a suitable surgical option, especially in patients who do not want extensive surgery.
Although the core extirpation method cannot completely eradicate the lesion or halt its progression, our results showed that AP/ML discrepancies remained stable for up to 4 years after the initial operation. Therefore, routine CT scans for lesion follow-up may not be necessary during the first 4 to 5 years unless the patient reports symptoms or noticeable facial contour changes. This is particularly important in pediatric patients who are more sensitive to radiation exposure.
Several limitations should be acknowledged in this study. First, the sample size was small, which precluded statistical analysis. In addition, the retrospective design of the study is a further limitation. Future randomized studies with longer follow-up periods are necessary to fully evaluate the long-term effectiveness of the core extirpation method. In conclusion, our preliminary results after 4 years of follow-up indicate that the core extirpation method may be a promising alternative for well-selected patients.