INTRODUCTION
A blue nevus is a neoplasm composed of pigmented dendritic dermal melanocytic cells in the reticular dermis. There are three types of benign blue nevi (common blue nevus, cellular blue nevus, and combined blue nevus) in addition to malignant blue nevi [1]. Plaque-type blue nevus (PTBN) is a variant of blue nevus [2]. PTBN is found at birth or arises in early childhood, and it shows a combination of the features observed in common blue nevus and cellular blue nevus. Herein we report an 88-year-old female patient who developed malignant melanoma in the setting of a PTBN.
CASE REPORT
An 88-year-old woman with no significant medical history presented with an enlarging plaque on her right cheek (Fig. 1). In a clinical examination, a blue maculo-papular confluent plaque was seen on the patient’s right cheek. The lesion was irregularly shaped, patchy or macular, and pale blue to blue-black. Skin biopsy was performed at our dermatology clinic. Histopathologically, the lesion had a collection of dendritic melanocytes in the dermis, and it was reported as “plaque-type blue nevus.”
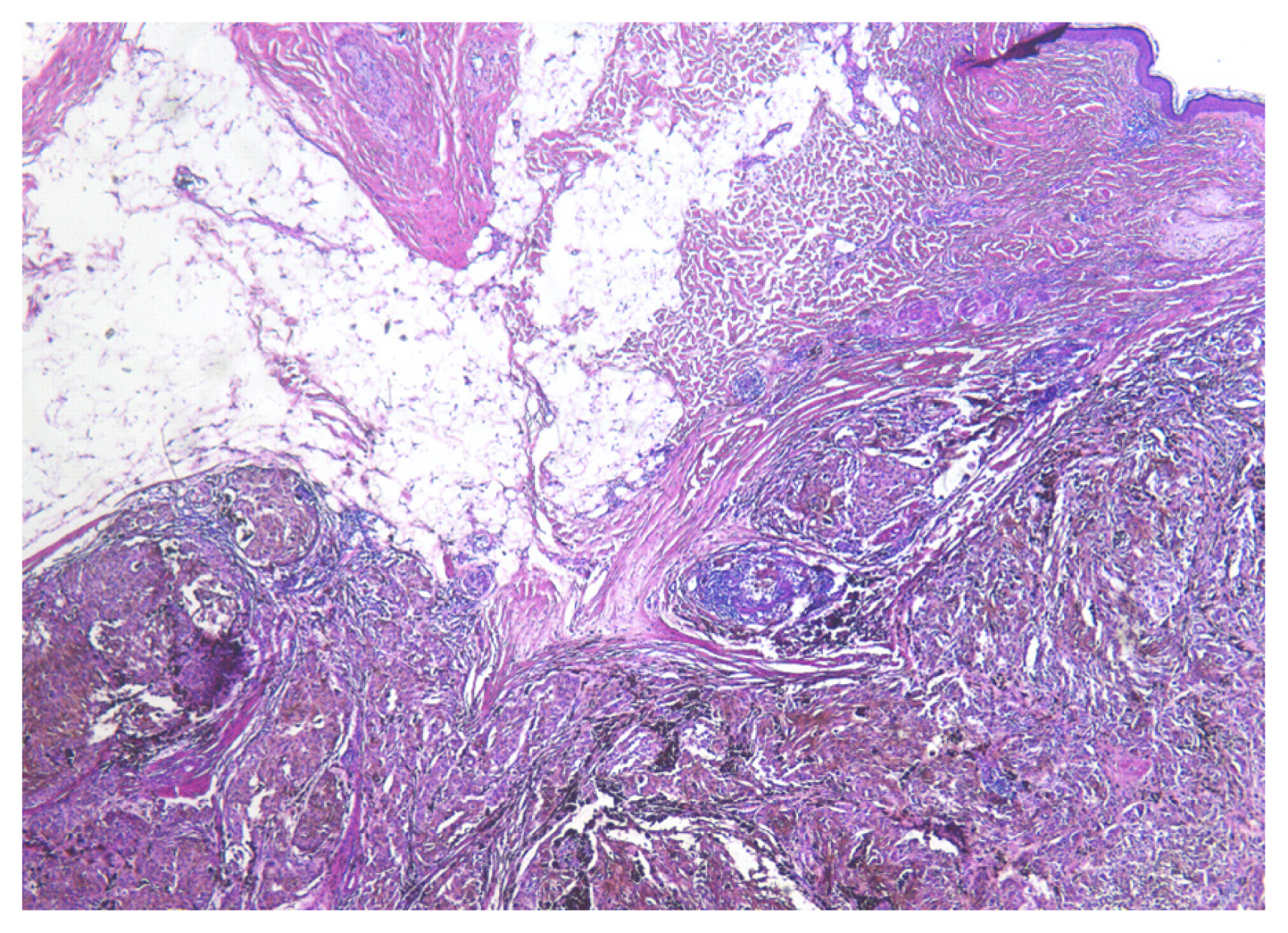
The lesion was removed by surgical excision. After surgical excision, the skin and soft tissue were covered by a split-thickness skin graft. After the operation, the patient healed well without any complications. However, a histopathological examination of the excised tissue showed atypical fusiform and epithelioid melanocytes containing granular or dense melanin pigment, which extended from the lower dermis to the subcutaneous layer. An immunohistochemical examination showed that the tumor cells and melanocytes were positive for HMB-45, MART-1, and S-100. The Ki-67 proliferation index was approximately 50% (Fig. 2). This constellation of findings was most consistent with a malignant melanoma arising in association with PTBN. According to the pathology report, the specimen was diagnosed as a malignant melanoma associated with PTBN. Tumor components were present in the resection margin. The invasion depth was 11 mm and there was no ulcerative lesion, so the tumor staging was T4a.
After the diagnosis of malignant melanoma associated with PTBN, enhanced computed tomography (CT) and magnetic resonance imaging (MRI) were performed. The mass showed high intensity on T1-weighted MRI and various intensities on T2-weighted imaging. Both CT and MRI showed a soft tissue tumor on the right cheek area without bone invasion. The possibility of metastasis was ruled out by a work-up that included chest CT, whole-body positron emission tomography-CT, a bone scan, and neck CT. We planned a second operation, which was performed under general anesthesia 22 days after the first surgery. Wide excision with supraomohyoid neck dissection and superficial parotidectomy were performed. The invasion depth was 11 mm and the safety margin was set to 2 cm [3,4]. The lymph node biopsies were negative for metastasis. The excised specimen was sent to our department of pathology for a histological examination of the biopsy. An analysis of the frozen-section biopsy showed that all margins were negative for malignancy. After wide excision, a skin and soft tissue defect measuring approximately 8×6 cm was present on the right cheek. The large defect was covered by a left lateral forearm free flap (Fig. 3) [5]. After the second operation, the patient received follow-up for 1 year without any sign of recurrence.
DISCUSSION
There are three types of benign blue nevi (common blue nevus, cellular blue nevus, and combined blue nevus), in addition to malignant blue nevus [6]. Common blue nevus, which is completely benign, is the most common subtype seen in the face [7]. However, cellular blue nevus may be locally aggressive and can persist or recur after complete excision. Furthermore, a few cases of cellular blue nevus metastasizing to the regional lymph nodes have been reported. Some studies have suggested that these cells do not represent true metastasis, but rather passive transport to the lymph nodes [8]. A malignant blue nevus was first described by Allen as a malignant melanoma originating from a preexisting blue nevus. However, in real-world practice, the distinction between a cellular blue nevus and a malignant blue nevus is equivocal, and considerable histopathological overlap may be present. This diagnostic problem has resulted in significant interobserver variability, even among experienced histopathologists, in the use and definitions of the term “atypical cellular blue nevus.”
PTBN is a rare variant of blue nevus, which was first described by Upshaw et al. in 1947 [9]. PTBN is present at birth or arises in early childhood, and may enlarge during puberty. It appears as a blue-gray pigmented area measuring 1 cm or more in diameter, and each lesion is composed of a single plaque or a confluence of several small macules or papules. Histologically, PTBN shows a combination of features found in common blue nevus and cellular blue nevus; there is no significant cytologic atypia, and mitotic activity is rare. Islands of heavily pigmented melanocytes mixed with collagen fibers extend to the deep subcutaneous layer [10,11]. A previous case of PTBN on the cheek was reported, which appeared as a bluish patch, as in our patient.
Rare cases with features similar to PTBN have been reported as “congenital segmental dermal melanocytosis,” characterized by a congenital onset and large bluish pigmentation of the chest or trunk; these lesions were common blue nevi, although one case was associated with cellular blue nevus [12]. These findings may be regarded as being within the spectrum of PTBN. Zattra et al. [13] reported an atypical blue nevus associated with a large PTBN. Until this diagnosis was confirmed, the patient reported a history of twice-recurrent nodules within pigmented lesions over 11 years, which were diagnosed as atypical blue nevus and melanotic schwannoma by biopsy. Another case report described a metastasizing and lethal melanoma arising in a large PTBN, thereby showing that some nodules in this setting are fully malignant. The clinical course of this patient was characterized by repeated local soft tissue recurrence over two decades and the absence of lymph node metastasis. Therefore, cases of atypical and malignant changes of PTBN have been occasionally documented, with a quite distinctive clinical course that is indolent but persistent [14]. There is no consensus among dermatopathologists regarding the precise distinction between PTBN and malignant melanoma associated with PTBN [15]. According to some authors, malignant melanoma associated with PTBN is a distinct variant of PTBN wherein subcutaneous nodules develop many years after PTBN has appeared.
However, Busam et al. [7] considered that their case of a lesion with nonpalpable nodules and deep subcutaneous foci characteristic of cellular blue nevus was malignant melanoma associated with PTBN. There is also debate about whether malignant melanoma associated with PTBN can appear de novo. In some cases, PTBN is characterized by areas resembling a common blue nevus and areas resembling a cellular blue nevus. Malignant melanoma associated with PTBN is characterized by histological features involving large areas of crowded, predominantly epithelioid cells and an infiltrative pattern with dense nodular collections. However, some authors do not accept this new entity and consider it only a semantically inconsequential terminological difference [14].
These lesions commonly appear stable and frequently have benign histological reports. The potential of malignant melanoma associated with PTBN was first reported in 2012, and whether this lesion represents a lesion with similar biological behavior to malignant blue nevus or to a conventional malignant melanoma remains a matter of debate [16]. Malignant blue nevus is usually considered to be more aggressive than conventional malignant melanoma, with tumor thickness and the largest tumor dimension showing potential correlations with the clinical outcome, but other studies have shown no biological differences when the tumors were matched with conventional malignant melanomas for Breslow depth, ulceration and other factors [17]. It is not surprising that the prognostic indicators of malignant melanoma associated with PTBN are difficult to predict, given the frequent large size, deep infiltration, and excessive rarity of these lesions. Malignant melanoma associated with PTBN is usually indolent, but may be regarded as a highly proliferative or true low-grade melanocytic malignancy that can evolve to a higher grade of aggressive malignancy and invasion. Malignant melanoma associated with PTBN exhibits slow local growth and a tendency to develop local recurrence or distant metastasis even after surgery. Nonetheless, the real level of risk for malignant melanoma and its prognostic factors are still unclear due to a lack of data. To our knowledge, this is the first reported case of malignant melanoma associated with PTBN in the cheek. The early surgical removal of such a nevus should be considered when subcutaneous nodules develop, owing to their potential for malignant transformation [18,19]. Long-term monitoring is required regardless of whether surgery is conducted. However, more data on the long-term prognosis and natural history of these lesions are required.
In conclusion, we report an unusual melanocytic tumor of the cheek, which was interpreted as a malignant melanoma arising in association with a PTBN. Our patient has had 1 year of being disease-free, but an uneventful postoperative course does not exclude the future potential for recurrence. The appropriate clinical management should involve frequent, long-term follow-ups.