INTRODUCTION
The forehead is anatomically the upper third of the face [1]. The frontalis muscle, one of the bellies of the occipitofrontalis, is one of the forehead muscles [2]. This muscle functions to elevate the eyebrow and horizontal wrinkles of the forehead [3].
Facial aging is a dynamic process that includes all tissue layers such as facial fat, facial bones, ligaments, muscles, and skin. The incidence and progress of the aging process vary in speed and severity from person to person [4]. Deep skin wrinkles can visually indicate the aging of the forehead. To elevate the eyelid tissue or sagging eyebrows in excess, the eyebrow-eyelid complex usually rises compensatively, resulting in chronic contraction of the frontalis muscle and the formation of wrinkles [5].
To prevent skin aging, research on skin rejuvenation is being actively conducted. Both surgical and nonsurgical approaches have been used to prevent facial aging [6]. The use of botulinum neurotoxin or a variety of fillers is one of the representative methods of skin rejuvenation.
Botulinum toxin was approved for temporary improvement of glabellar lines and has been used widely for various aesthetic purposes [7].
There are currently only two serotypes of neurotoxin available. Various botulinum toxins have been developed and marketed, including Botox (onabotulinumtoxinA) and Dysport (abobotulinumtoxinA). In 2000, the Food and Drug Administration also approved Myobloc (rimabotulinumtoxinB). Xeomin (incobotulinumtoxinA) was introduced 2005 [8].
Double-blind, split-face studies are being actively conducted to analyze the effects of drugs [9,10]. The split-face study in which the drug is administered by dividing the forehead area of the test subject in half was conducted to directly compare the effects of facial rejuvenation at a certain time after botulinum toxin administration. In this study, we investigated whether the split-face study is a reliable method for botulinum toxin research by comparing right and left eyebrow heights and movements, and the electromyography (EMG) signal of the frontalis muscle. In addition, by comparing the data of the study subjects, we examined the relationship between eyebrow movement and EMG muscle activity, changes in the right and left eyebrow heights and movements, and EMG muscle activity with age.
METHODS
This study was approved by the Institutional Review Board of Gachon University Gil Medical Center, Republic of Korea (IRB No. GCIRB 2014-360). All the subjects signed a consent form, and the study was conducted in accordance with the principles of the Declaration of Helsinki.
The subjects were 31 women between 35 and 55 years of age. The exclusion criteria were as follows: patients who had received botulinum toxin injection, treatment with fillers or laser resurfacing within 24 months, and treatment with hyaluronic acid or other fillers within 12 months, and those with scars or marked asymmetry in the forehead region.
We measured eyebrow height and eyebrow movement, and EMG signal. Eyebrow height was defined as the distance (mm) from the eyebrow to the upper eyelid margin at primary gaze and measured on both sides. Eyebrow movement was measured as the distance (mm) the eyebrows moved by grimacing the forehead for 5 seconds. EMG studies were conducted on the frontalis muscles by using the BioPak system (BioResearch, Inc.). Electrode skin areas were cleaned before electrode placement. The reference electrode was located on the chin and measurement electrodes were attached to the center of the frontalis muscle, which is in the middle between the hairline and eyebrow above the pupil. The subjects were asked the forehead muscle was contracted to raise the eyebrow as far as possible. A specialist of rehabilitation medicine conducted the EMG tests and measured the waveform of the EMG. The data points were the average value of the maximal amplitude of the surface EMG muscle activity that appeared when the subjects contracted the frontalis muscle three times at maximum voluntary contraction.
Statistical analyses
The paired t-test was used to compare the eyebrow height and eyebrow movement between the right and left and the EMG values of the right and left frontalis muscles. We used the Pearson correlation analysis to study the correlation between eyebrow movement and EMG muscle activity and the changes in right and left eyebrow heights, movements, and EMG value with age. All statistical analyses were performed using SPSS Version 20 (IBM Inc.). A value of p<0.05 indicated statistical significance.
RESULTS
Patient demographics
The study was conducted in 31 women with ages ranging from 35 to 55 years. The mean age of the group was 42.94±5.51 years.
Eyebrow height
The mean eyebrow heights of the right and left eyes were 13.24 and 13.55 mm, respectively. No statistically significant differences were found in the right and left eyebrow heights (p=0.256) (Table 1).
Eyebrow movement
The distance of the eyebrows was measured by frowning the forehead, and the mean distances on the right and left sides were 7.68 and 7.68 mm, respectively. No statistically significant differences were found in the right and left eyebrow movements (p=1.000) (Table 1).
EMG muscle activity of the frontalis
The mean frontalis muscle EMG values on the right and left sides were 181.90 and 181.79, respectively. No statistically signif-icant difference was found between the two groups (p=0.978) (Table 1).
Change in eyebrow height with age
The correlation coefficient between age and eyebrow height was 0.078, but not statistically significant (p=0.560).
Change in eyebrow movement with age
By comparing eyebrow movement according to age, we found that the correlation coefficient is –0.032, but the correlation was not statistically significant (p=0.814).
EMG waveform with age
The results of the EMG waveform with age were as follows: Analysis did not show any association with a correlation coefficient of 0.000 and was not statistically significant (p=0.999).
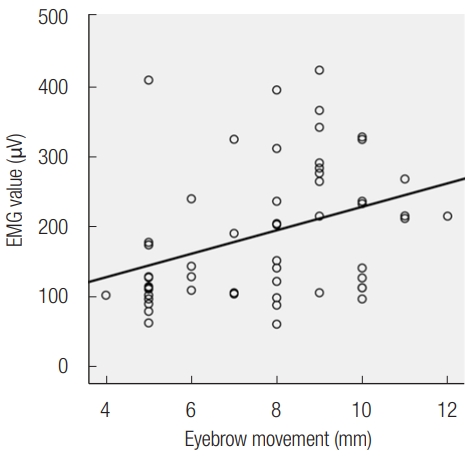
Relationship between EMG muscle activity and eyebrow movement
The EMG value had a weak positive linear association with the movement of the eyebrow with a correlation coefficient of 0.366 and was statistically significant (p<0.001) (Fig. 1).
DISCUSSION
Commercially available botulinum toxin formulations for treatment of dystonia in the United States include onabotulinumtoxinA (OnaBoNT-A), abobotulinumtoxinA (AboBoNT-A), incobotulinumtoxinA (IncoBoNT-A) and rimabotulinumtoxinB (RimaBoNT-B). Several botulinum neurotoxin formulations, including prabotulinumtoxina A-xvfs, daxibotulinumtoxin A (DaxiBoNT-A), neu-botulinumtoxinA (NeuBoNT-A), letibotulinumtoxin A, botulinum toxin E (rBoNT-E), Innotox, and QM-1114 are currently used in many countries, even though are not approved by Food and Drug Administration for the treatment of dystonia [11]. New botulinum toxins are continuously being developed, and split studies are being conducted to compare them with existing products. Botulinum toxin exists in seven types of neurotoxins (types A–G) [12]. A split-face study is being conducted to compare the effects of each type of botulinum toxin [13,14].
Meanwhile, the reliability of split-face studies of botulinum toxin is controversial. Studies have been conducted to address the unwanted side effects of the diffusion of botulinum toxin. Animal electrophysiological studies have shown that non-target muscles are affected by botulinum toxin injection. According to a study by Yaraskavitch et al. [15], when measuring force production and the muscle weakness of the target and adjacent non-target muscles after botulinum toxin injection, both muscle groups exhibited decreases regardless of the target. The result indicated that botulinum toxin can pass through the muscle fascia and reach adjacent muscles, causing muscle weakness [16]. The spread of botulinum toxin tends to be caused by the diffusion of unbound toxins through the extracellular space. This is caused by the concentration gradient and dynamics of the injection [17].
Measurements of the compound muscle action potential (CMAP), an indicator of efficacy and diffusion, showed a reduction not only in the ipsilateral but also in the contralateral glabellar muscles when on botulinum toxin A was injected in the corrugator muscle unilaterally [18]. In Girlanda et al. [19], single-fiber EMG signals and CMAP were measured in the orbicularis oculi muscles when botulinum toxin was injected in one eye and saline solution was injected in the other eye. As a result, facial CMAP decreased bilaterally, and the single-fiber EMG signal changed statistically significantly on both sides [19]. Therefore, the dilution and injection capacity must be adjusted because the injected botulinum toxin can spread and affect the opposite area.
Weise et al. [20] suggest that botulinum toxins not only affects neuromuscular junctions but may also have central effects on the central nervous system. In addition, botulinum toxin may affect antagonist muscles and other noninjected muscles in addition to the corresponding muscles. According to Matak [21], an axonally transported botulinum toxin mitigates muscle hypertonia caused by tetanus toxin. This process is attributed to the transsynaptic movement of botulinum toxin in the central nervous system.
We used surface EMG to measure the electrical activity of muscles from the body surface. Surface EMG, which is used by attaching an electrode to the skin surface, has the advantage of being able to measure temporary high-resolution muscle electrical activity and detect quickly and in a short period [22]. The main advantage of surface EMG is that it is noninvasive and painless, unlike using a needle. This method is also used in facial studies and diagnosis of facial myopathy or neuropathy because the EMG signal constantly changes with muscle movement [23-25].
In this study, we showed no significant differences in eyebrow height and movement, and EMG muscle activity on the right and left sides. Based on the comparison of data between study participants, no significant relationship was found between age and each indicator, but a significant result was obtained between eyebrow movement and EMG muscle activity. The EMG signal was positively associated with eyebrow movement by Pearson correlation analysis.
In conclusion, we demonstrated the reliability of the split study by finding no difference in eyebrow height or movement between the left and right sides. We also found a positive correlation between EMG of the frontalis muscle and eyebrow movement, proving the usefulness of EMG in rejuvenation research.