Facial artery: anatomical variations in the perioral region in cadavers
Article information

Abstract
Background
In recent years, there has been an increase in reports of perioral vascular complications resulting from filler injections, such as necrosis of the lip or alar rim, occlusion, and in severe cases, blindness. Conversely, the use of perioral arterial flaps is becoming more prevalent in the treatment of cleft lips, cancer, and trauma. A thorough understanding of perioral arteries is essential to minimize complications and maximize the success of these flaps. However, the course of the facial artery (FA) in the perioral region remains incompletely understood. The aim of this study was to describe the variations of the FA in the perioral region.
Methods
We dissected 52 embalmed and formaldehyde-fixed Vietnamese cadavers. We then studied the size and distribution of perioral arteries in 102 specimens.
Results
The superior labial artery (SLA) was the most common branch, occurring in 87.25% of cadavers, followed by the inferior labial artery (ILA) at 78.43%. The SLA primarily originated above the mouth corner (cheilion), accounting for 91.01% of cases, and predominantly exhibited a tortuous course within the submucosa (78.65%). The ILA’s branching pattern varied, but it was primarily located below the cheilion (91.25%). The ILA also followed a twisted path, generally within the submucosa. The ILA exhibited two patterns: the typical pattern, distributed at the vermilion border of the lower lip (8.82%), and the horizontal labiomental artery pattern, which ran horizontally in the middle of the lower lip area (69.61%). At their origin, the SLA and ILA had average external diameters of 1.29 mm and 1.28 mm, respectively.
Conclusion
Numerous anatomical variations in the FA in the perioral region were found. A detailed anatomic description, suggested landmarks, and angiography before the procedure will be useful to help doctors avoid complications.
INTRODUCTION
Dermal fillers are widely used to enhance, rejuvenate, and contour the face, with the lips being the most common site for facial volumizing procedures. However, improper handling can lead to perioral vascular complications, including lip and alar rim necrosis, occlusion, and in severe instances, blindness. Various concepts of the facial artery (FA) perforator flap have been proposed to provide greater flexibility in reconstructing perioral deficiencies caused by cleft lip, cancer, or trauma injuries. The primary arteries supplying the perioral region are the superior labial artery (SLA) and the inferior labial artery (ILA). Ensuring an adequate blood supply is crucial to the success of these flap surgeries; hence, the perioral arteries should be effectively included into the pedicle [1,2].
The SLA, which originates from the FA, runs along the vermilion border of the upper lip. The FA provides blood supply to the lower lip via the ILA [3]. Recent anatomical studies have identified two distinct patterns followed by the ILA. The first pattern diverges from the FA at the cheilion (the corner of the mouth, or oral commissure) and runs parallel to the vermilion border of the lower lip. The second pattern, in contrast, runs below the cheilion and continues along the labiomental crease, distinguishing it from the typical ILA. This branch is also referred to as the horizontal labiomental artery (hLMA). The vertical labiomental arteries are formed either by several vertical branches of the hLMA anastomosing with the ILA that follows the first pattern, or by the submental artery. Most of the published data on the FA lacks detailed information about anatomical variations in the perioral region [4-10].
As a result, the purpose of this research is to present the perioral arteries and their relationship to anatomical landmarks.
METHODS
The FA was dissected in 52 adult Vietnamese cadavers that had been embalmed and fixed with formaldehyde at the Anatomy Department, University of Medicine and Pharmacy, Ho Chi Minh City, Vietnam.
A total of 102 hemifaces from 52 cadavers were dissected, none of which exhibited craniofacial abnormalities. The dissections were performed under × 2.5 loupe magnification, following the procedures outlined in Cunningham’s Manual of Practical Anatomy. A midline incision was made to carefully reflect the skin, platysma, and superficial fascia over the carotid triangle on each side of the neck and face. Upon reflection of the deep cervical fascia, the superior belly margins of the sternocleidomastoid and omohyoid muscles were delineated. The submandibular gland was mobilized after the margins of the posterior bellies of the digastric and stylohyoid muscles were defined. The carotid sheath was then opened within the carotid triangle, allowing for the identification of the external carotid artery and its branches. The FA, the third branch of the external carotid artery in the neck, was identified and traced from its origin to its termination. The branching pattern of the FA, particularly its termination in the perioral arteries, and its relationship to anatomical landmarks were noted. The origin of the SLA, denoted as point S, was determined in relation to a plane defined by two axes running through the corners of the mouth (point O): the horizontal axis Ox (from the left cheilion to the right cheilion) and the vertical axis Oy (parallel to the sagittal midline).
RESULTS
From 52 adult Vietnamese cadavers, 102 FAs were dissected (average age at death: 74.31 years; age range: 32–100 years; 17 females and 35 males). The FAs were dissected from both the left and right sides of 50 cadavers, while in two cadavers, dissection was performed only on one side (one on the left and one on the right) due to tissue damage.
The FA terminated as the angular artery (AA) or forehead branch in 33 cases (32.4%), as the lateral nasal artery (LNA) in 33 cases (32.4%), as the inferior alar artery (IAA) in seven cases (6.9%), as the SLA and ILA in 4.9% (5/102) of cases. Duplexes were found in 17.6% (18/102) of FAs. In one case (1%), the FA had a short course and terminated under the inferior labial region. The AA can be classified into three types: the typical AA, which runs along the lateral side of the nose (21 cases, 20.6%); the orbicularis oculi muscle (OOc) AA, which runs along the lower border of the OOc (10 cases, 9.8%); and the F (2 cases, 2%) (Fig. 1).
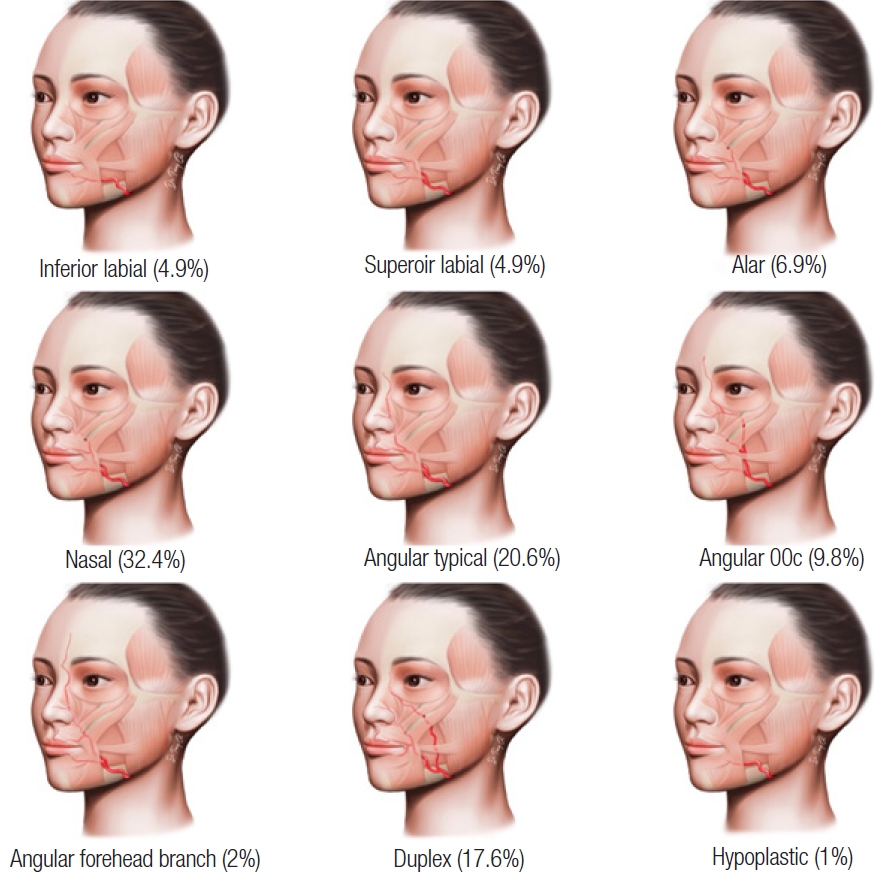
Branching patterns according to the termination of 102 facial arteries in our study OOc, orbicularis oculi muscle.
The SLA was the most prevalent branch among the 102 FAs, representing 89 of the cases (87.25%). This was followed by the ILA with 80 (78.43%), the LNA with 67 (65.69%), the IAA with 59 (57.84%), the typical AA with 21 (20.59%), the AA-OOc with 10 (9.8%), the forehead branch with two (1.96%), and the duplex with 18 (17.65%). In one instance (0.98%), the FA had a brief trajectory in the labiomental region.
The SLA was visible in 89 cases. In seven cases (7.87%), the SLA was only visible on the right side, while in six cases (6.74%), it was only visible on the left side. In 76 cases (85.39%), the SLAs were visible bilaterally. In 13 cases where the SLA was absent, the upper lips were vascularized by the contralateral SLA arteries (11 cases) and the transverse FA on the same side (2 cases).
The SLA originated above the cheilion in 91.01% of cases (81/89). In seven cases (7.87%), it originated at the cheilion, and in one case (1.12%), it originated below the cheilion. In 73 out of 89 cases (82.02%), the SLA originated lateral to the cheilion, while in 16 out of 89 cases (17.98%), it started medial to the cheilion. The average distance from the initial point of the SLA to the cheilion was 8.83 mm above, 8.39 mm lateral, and 8.13 mm medial, respectively. The origin of the SLA, referred to as point S, was found in 78.65% of cases (70/89) within a square measuring 1.5 cm on each side, located superolateral to the cheilion (Fig. 2).
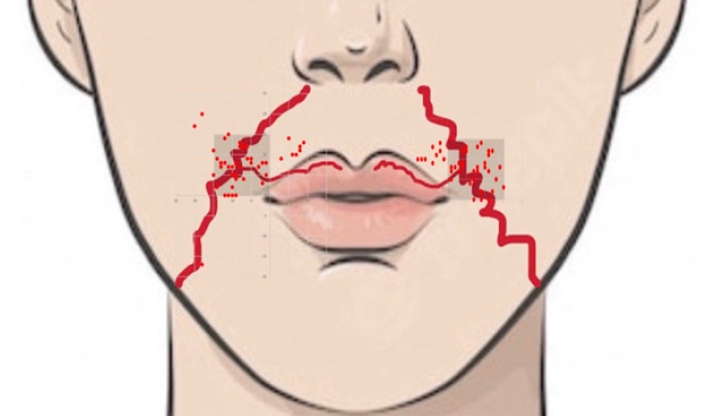
The origin of the superior labial artery (S point: red dots) in our study.
The SLA followed a serpentine path, anastomosing with the opposite artery in the middle of the upper lip. The SLA was more superficial in the midline. On both the left and right sides of the same cadaver, the SLAs were markedly different and asymmetrical. The SLA traversed between the oral mucosa and the OOc in the submucosa, within the muscle (intramuscular), or between the muscle and the skin (subcutaneous) in 78.65%, 17.98%, and 3.37% of cases, respectively. Notably, the SLA changed planes during its course: 15.69% changed once, and 2.94% changed twice.
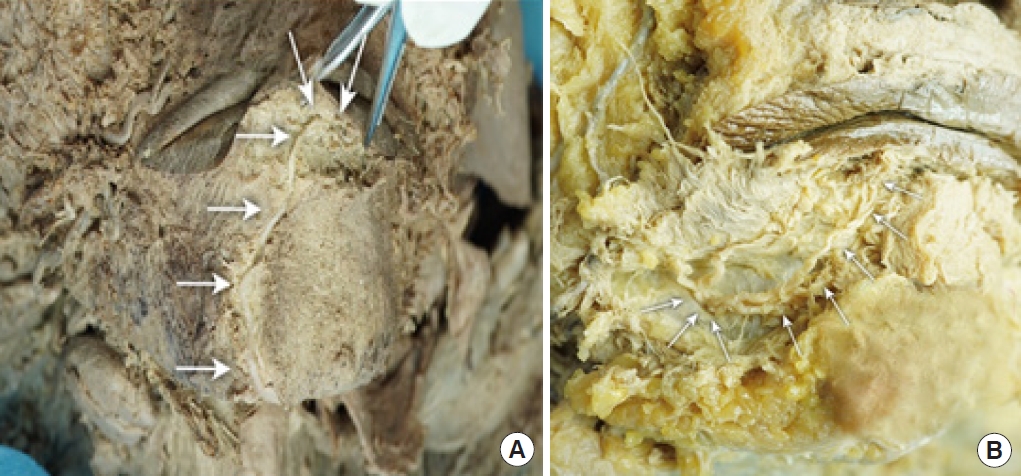
Every SLA provided at least one nasal septal branch to the nasal septum. Out of 102 FAs, 20 had SLAs that did not have an IAA or inferior alar branch. Six out of 102 SLAs gave off IAAs, as shown in Fig. 3. One IAA originated directly from the FA without an SLA. Four IAAs originated from the opposite side of the SLAs, two cases from the opposite side of the LNA, and one case from the infraorbital artery. Thirteen out of 102 IAAs did not originate directly from the FA.
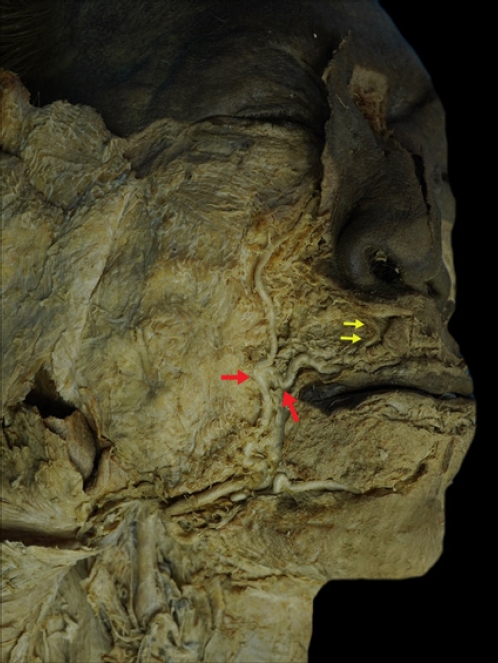
Superior labial artery (red arrows) with inferior alar artery (yellow arrows) in a cadaver.
The ILA was visible in 80 cases. In 22 cases, it was only visible on the right side, while in 18 cases (22.5%), it was visible on the left side. Bilateral visibility was observed in 40 cases (50%). Of the 40 unilateral ILAs, 38 supplied blood to the entire lip. In two instances, the arterial supply of the lower lip did not originate from the FA: one case involved the mental artery and the other involved the submental artery (Figs. 4, 5). The branching of the ILA varied between the lower border of the mandible and the corner of the mouth: it was primarily below the cheilion in 73 out of 80 cases (91.25%), at the level of the cheilion in six out of 80 cases (7.5%), and above the cheilion in one case (1.25%). The ILA exhibited the first typical ILA pattern in 8.82% of cases (9/102) and the second pattern, known as the hLMA, in 69.91% of cases (71/102) (Fig. 6). The hLMA was present in 37.25% of cases (38/102). The ILA also followed a serpentine pattern and anastomosed with the contralateral artery. The ILA was located submucosally, intramuscularly, or subcutaneously in 81.25%, 16.25%, and 2.5% of cases, respectively.
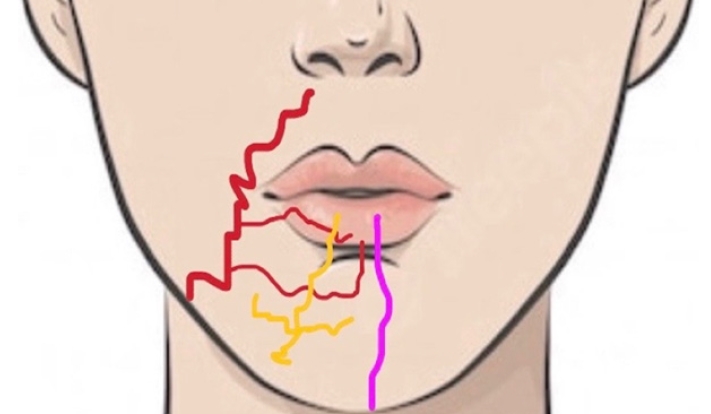
Arterial sources in the lower lip. Red lines: inferior labial artery+horizontal labiomental artery from the facial artery, yellow lines: mental artery, violet line: ascending mental branch from the submental artery.
Unusual arterial sources in the lower lip in a cadaver. (A) Ascending mental branch from the submental artery (arrows). (B) Mental artery (arrows).
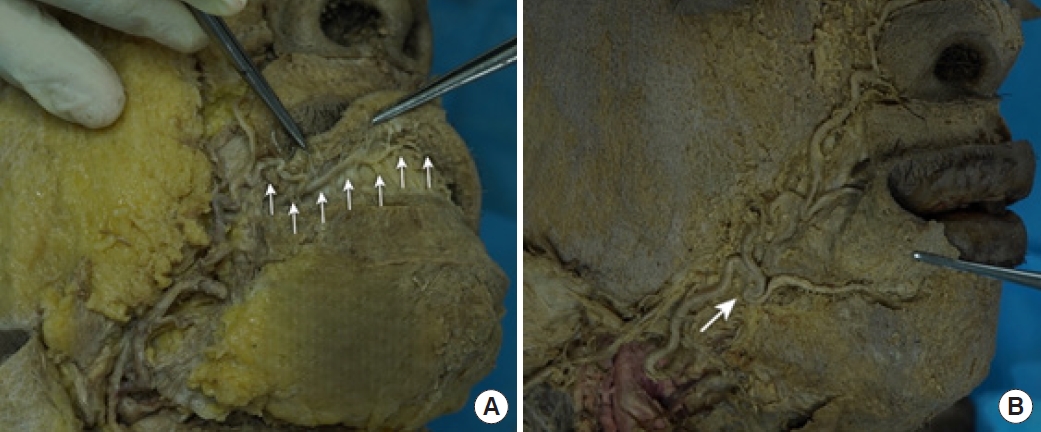
Inferior labial artery (ILA) in a cadaver. (A) Typical ILA (arrows). (B) ILA with a horizontal labiomental artery pattern (arrow).
At their origin, the SLA and ILA had average external diameters of 1.28 ± 0.64 mm (0.31–2.55 mm) and 1.29 ± 0.07 mm (0.31–2.54 mm), respectively. We observed statistically significant differences in these external diameters when comparing by side and gender (p< 0.05). However, there were no statistically significant differences in age range or by termination point of FA (p> 0.05).
DISCUSSION
In our study, we observed the SLA on the right side in seven cases (7.87%), on the left side in six cases (6.74%), and bilaterally in 76 cases (85.39%). Park et al. [11] found that the SLA was present bilaterally in 90% of cases, giving rise to superficial and deep septal branches. Magden et al. [12] reported a bilateral presence in 71% of cases and a unilateral presence in 29% of cases. In contrast, Furukawa et al. [13] found the SLA visible only on the right side in 30.3% of cases, on the left side in 10.6%, and bilaterally in 53% of cases. Therefore, the SLA can manifest in a range of unilateral and bilateral locations.
The SLA originated above the oral commissure in 91.01% of cases. Various studies have summarized the origin of the SLA relative to the oral commissure, as shown in Table 1. Our findings align with those of Pinar et al. in 2005 [5] and Al-Hoqail and Meguid in 2008 [7], but differ from those of Loukas et al. in 2003 [6]. The S point (origin of the SLA) was identified in 78.65% (70/89) of cases within a 1.5 cm square located superolaterally to the cheilion. Lee et al. [14] reported a similar finding in 85% of cases. According to our study, the cheilion can serve as a soft tissue landmark for locating the S point, which is typically found 8–9 mm above, and either lateral or medial to it. FA perforators appear to be most common in the region 1–2 cm lateral to the cheilion [14].

Summary of studies on the origins of the SLA in relation to the oral commissure
Lee et al. [14] proposed a four-category classification of the SLA, with each type defined by its relationship with the FA trunk. Type I: the FA independently gives rise to the SLA and alar branch (56.7%, 34/60). Type II: The alar branch originates from the SLA (21.7%, 13/60). Type III: The FA terminates as the SLA (15.0%, 9/60). Type IV: the SLA is absent (6.7%, 4/60). In our study, the results were as follows: type I: 58/102 (56.86%), type II: 6/102 (5.88%), type III (the FA terminates as the SLA): 5/102 (4.9%), type IV (the SLA is absent): 13/102 (12.75%). In 20 out of 102 cases (19.61%), the SLAs did not fit into any of the four types, with the FA giving rise to the SLA without the IAA.
A total of 80 ILAs were observed, with 42 cases on the right side and 38 cases on the left side. The ILA was only visible on the right side in 22 cases (27.5%), on the left side in 18 cases (22.5%), and bilaterally in 40 cases (50%). Pinar et al. [5] reported a unilateral presence of the ILA in 10% of their specimens, and a bilateral presence in 90% of their specimens. Edizer et al. [15] found the ILA unilaterally in 64% of specimens and bilaterally in 36%. Furukawa et al. [13] observed the ILA only on the right side in 47.3% of cases, on the left side in 16.5%, and bilaterally in 16.5%. In conclusion, both the ILA and SLA were unilateral in some instances. The presence of these arteries should be confirmed before designing a flap supplied by them for surgery.
The ILA mostly originated below the oral commissure (91.25%). This finding is not consistent with the results reported by other authors [5,7]. The origin of the ILA in relation to the oral commissure, as reported by various studies, is summarized in Table 2.
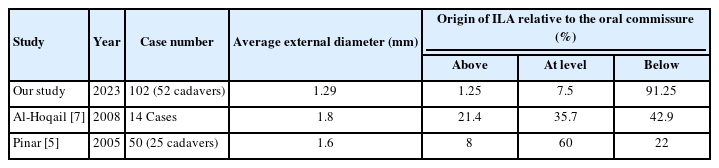
Summary of studies on the origins of the ILA in relation to the oral commissure
The second pattern of ILA (hLMA) was observed in 52.4% of cases according to Lee et al. [16], and in 69.61% of cases in our study. Therefore, the presence of the ILA near the vermilion border of the lower lip is not guaranteed. Angiography of the ILA should be performed prior to any procedure involving the lower lip. Given these distribution patterns, the approach to flap design during lower lip reconstruction should deviate from traditional methods. The ILA in the second pattern, hLMA, should be considered as grafted into the pedicle. The area below the cheilion can be utilized as donor sites for the hLMA-free flap in lip reconstruction.
In our studies, the ILAs originated from three sources: from the FA in 80 cases, from the mental artery in one case, and from the submental artery in one case. In a separate study, Tansatit et al. [17] reported five origins based on 11 cadavers and 20 volunteers. Type 1, the labiomental branch, was found in 15 of 49 cases (30.6%). Type 2, the modiolar branch, was found in 12 of 49 cases (24.5%). Type 3, the ascending mental branch, was also found in 12 of 49 cases (24.5%). Type 4, the FA branch, was found in five of 49 cases (10.2%). Lastly, type 5, the superior labial branch, was found in five of 49 cases (10.2%). The vascular system of the lower lip is very rich. With this understanding, we can utilize a variety of flap types with these arterial pedicles. Concurrently, physicians must exercise particular caution when performing cosmetic injection procedures in the lower lip region to prevent damage to the blood vessels.
The depth of the SLA has been summarized in various studies, as shown in Table 3, and corresponding results for the ILA are presented in Table 4. These arteries are located submucosally, with the SLA at 78.65% and the ILA at 81.25%. This finding aligns with the results of other authors, including Cotofana, Loukas, Pinar, Ahmadi, and Lee [5,6,9,18-20]. Lee et al. [20] also reported that the labial arteries were predominantly found in the wet mucosal layer at most reference points on the upper lips (35%–57%) and lower lips (28%–55%). The paths of the SLA and ILA can be critical for enhancing lip volume with filler. Given this anatomical evidence, we should inject local anesthetic drugs or filler very superficially into the vermilion border during lip injections to prevent tissue ischemia and/or excessive bruising. Conversely, the SLA and ILA appear more superficially in the midline, which is particularly important for volumetric enhancement of the upper lip and Cupid’s bow region. However, the course of the FA in the perioral region varies significantly among individuals. Therefore, caution must be exercised regarding the depth of the vessels to avoid injury and vascular damage. The SLA and ILA traverse and anastomose with the opposite artery in the middle. Based on this current information, the reverse SLA island flap has been suggested as a potential reconstructive treatment for nose and cheek deficiencies [21].
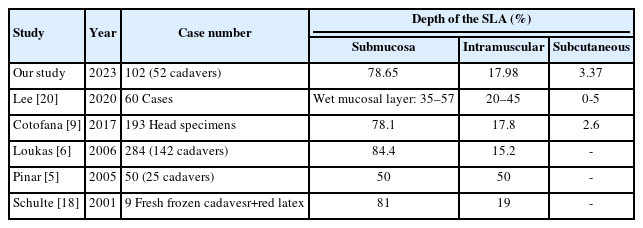
Summary of the depth of the SLA as described in the literature

Summary of the depth of the ILA as described in the literature
The course, appearance, and position of the labial arteries exhibit significant variation among different individuals and even between different sides within the same individual. It is crucial to be cognizant of these anatomical variations in artery location, not only for dermal filler injections but also for other injectable treatments or flaps targeting the upper lip area. The arteries within the human lip vascular system are highly variable and exhibit a low degree of symmetry. Providing a detailed anatomical description, suggesting landmarks, and performing angiography prior to the procedure can assist physicians in minimizing the risk of vascular complications such as necrosis and permanent blindness, thereby maximizing the success rate of perioral artery flaps.
Notes
Correction
This article was corrected on the reference list.
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Funding
This study was supported by the University of Medicine and Pharmacy, Ho Chi Minh City, Vietnam.
Ethical approval
This study’s protocols were approved by the University of Medicine and Pharmacy at Ho Chi Minh City 2 (No. IRB-VN01002/ IRB00010293/FWA00023448).
Author contributions
Conceptualization; Data curation; Formal analysis; Methodology; Project administration: all authors. Visualization: Vu Hoang Nguyen, Trang Huu Ngoc Thao Cai. Writing - original draft: Trang Huu Ngoc Thao Cai. Writing - review & editing: all authors. Investigation: all authors. Resources: Vu Hoang Nguyen, Trang Huu Ngoc Thao Cai. Software: Lin Cheng-Kuan, Trang Huu Ngoc Thao Cai. Supervision; Validation: all authors.
Abbreviations
AA
angular artery
FA
facial artery
hLMA
horizontal labiomental artery
IAA
inferior alar artery
ILA
inferior labial artery
LNA
lateral nasal artery
OOc
orbicularis oculi muscle
SLA
superior labial artery