Clinical characteristics of pediatric nasal bone fractures by age group
Article information

Abstract
Background
The clinical characteristics of pediatric nasal fractures can vary depending on the child’s age, social activities, and environment. Therefore, this study aimed to analyze these characteristics in different age groups.
Methods
We retrospectively reviewed of a series of patients aged under 12 years who received treatment between 2013 and 2021. The initial study design involved dividing the patients into four age groups, corresponding to different developmental ages, but there were no cases in infants aged 0 to 1 year. Therefore, the patients were divided into three groups: group I, between 2 and 5; group II, between 6 and 9; and group III, between 10 and 12 years of age. The following parameters were evaluated: sex, age, etiology, fracture type and severity, and the incidence of septal injuries.
Results
In total, 98 patients were included in this study. In group III, the ratio of boys to girls was 3.88:1, exceeding the overall ratio of 1.97:1. The most common cause varied with age: slipping down in group I, bumping accidents in group II, and sports accidents in group III. Concomitant septal injuries were present in 4.17% of patients in group I, 5.71% of patients in group II, and 28.21% of patients in group III.
Conclusion
Increasing age was accompanied by a greater tendency for male predominance and a higher prevalence of sports-related causes and septal injuries. Violence was infrequent but started to become a contributing factor during school age. These varying environmental factors across age groups can offer valuable insights into the epidemiology and clinical characteristics of pediatric nasal bone fractures.
INTRODUCTION
Significant differences exist in children’s anatomic characteristics, parental attention and care, social relationships, and social activities according to age, and the age of 12 years has been identified as a noteworthy transition point [1,2]. However, few studies have taken age-specific differences into account, especially in research on nasal bone fractures in pediatric populations. Therefore, the aim of this study was to analyze differences in the characteristics of pediatric nasal fractures in various age groups among children 12 years of age and younger.
METHODS
A retrospective review was conducted of the medical records of pediatric patients aged 12 years or younger who had isolated nasal bone fractures including septal fractures and underwent closed reduction. This study excluded patients with other facial fractures, previous nasal bone fractures, or congenital facial deformities.
Information was extracted on patients’ demographics, including sex, age, etiology, fracture pattern, and the presence of a septal injury. Fractures were evaluated using a dual 128-channel CT scanner (Somatom Definition Flash; Siemens), and the types of nasal bone fractures were classified using the system developed by Stranc and Robertson [3].
For the epidemiological analysis, we initially intended to study four distinct age groups: infants, the first growth period, kindergarten through lower primary school grades, and upper primary school grades. However, due to the absence of patients aged 0–1 year (n= 0), we categorized patients into three groups by developmental age: group I (first growth period), between ages 2 and 5; group II (kindergarten and lower grades of primary school), between ages 6 and 9; group III (upper grades of primary school), between ages 10 and 12 years. Environmental factors were evaluated by age group. Statistical analysis was performed using SPSS version 19.0 (IBM Corp.).
RESULTS
This study included 98 patients (65 boys and 33 girls). Group I (first growth period of the nasal bone) contained 24 patients (12 boys and 12 girls), group II included 35 (22 boys and 13 girls), and group III contained 39 (31 boys and 8 girls) (Table 1). The most common causes of injury were slipping down accidents (13 cases, 54.17%) in group I, bumping accidents (20 cases, 57.14%) in group II, and sports-related accidents (14 cases, 35.90%) in group III (Table 2).

Sex ratio according to age group

Etiology of nasal bone fractures in each age group
The number of patients with a plane I fracture pattern was 23 of 24 in group I (95.83%), 33 of 35 in group II (94.29%), and 32 of 39 in group III (82.05%). The overall incidence of plane I fracture patterns was 89.80%. The number of patients with concomitant septal injuries was one in group I (4.17%), two in group II (5.71%), and 11 in group III (28.21%) (Table 3).

Incidence of plane I fracture patterns and septal injuries by age group
DISCUSSION
Numerous studies have investigated the epidemiology of nasal bone fractures in pediatric populations. However, these studies have either categorized pediatric patients based on age groups relevant to the epidemiology of violence, such as preschool (0–5 years) and school age (6–11 years) [4,5], or they have concentrated on the causes and mechanisms of injury [6]. Another study examined the sex distribution and causes of injury in pediatric patients, dividing the subjects into four age groups (0–3, 4–6, 7–9, and 10–12 years). However, that study included all facial bone fractures, not exclusively nasal bone fractures. As a result, detailed age-specific information on nasal fractures in pediatric patients was not provided [7].
The initial peak growth of the nasal bone occurs between the ages of 2 and 5, followed by a period of gradual growth. During puberty, there is a second significant growth spurt in the bone, along with additional growth of the septum [8,9]. Furthermore, no study seems to have specifically investigated the epidemiology of nasal bone fractures during the critical growth period of the nose (2–5 years) in pediatric patients. With this in mind, we conducted a study on the epidemiology of nasal bone fractures, subdividing the pediatric population into the following age groups: early childhood (2–5 years), lower school age (6–9 years), and upper school age (10–12 years).
In addition, children of varying ages exhibit notable differences in anatomical characteristics, parental involvement in care, social relationship development, and areas of social activity. Hence, to account for age-related differences, we investigated the clinical characteristics of pediatric nasal bone fractures in infants, early childhood in the first growth period, children in kindergarten and the lower grades of primary school, and children in the upper grades of primary school. This study showed that the characteristics of nasal bone fractures vary significantly across pediatric age groups, and several noteworthy findings are discussed below.
The first point to note is that there were no patients who fell into the category of infants (aged 0 to 1 year). This may be attributed to the limited mobility of infants in this age group and the extensive care they typically receive from their parents.
Second, pediatric nasal fractures occurred more frequently in boys than in girls, with 65 cases (66.33%) in boys and 33 cases (33.67%) in girls. However, when analyzed by age group, the number of cases in boys was 12 (50%) out of 24 in group I, 22 (62.86%) out of 35 in group II, and 31 (79.49%) of 39 in group III. In this study, the incidence of nasal fractures was equal between boys and girls during the first growth period. However, by the time children reach the upper grades of primary school, the male-to-female ratio of nasal fractures increased to approximately 4:1, roughly equaling the ratio observed in adults [4,10]. The higher prevalence of nasal fractures among boys in the upper primary grades is thought to result from differences in social and sports activities between boys and girls [11]. This phenomenon becomes markedly more evident in adolescence, during which boys have been reported to account for approximately 90% of nasal fracture patients [12].
Third, regarding the etiology of nasal fractures in the pediatric population, a study conducted in Korea found that the predominant causes were falls or slip-down injuries [4,7]. Consistent with prior research, the primary causes of fractures among the overall pediatric population in this study were collisions with people or objects and slip-and-fall incidents, accounting for 33 (33.67%) and 28 (28.57%) cases, respectively. Other causes included sports-related accidents (19 cases), traffic accidents (10 cases), accidents related to social activities (3 cases), assaults (3 cases), and falls (2 cases).
The most common cause of injury was slipping accidents (13 cases, 54.17%) in group I, bumping accidents (20 cases, 57.14%) in group II, and sports-related accidents (14 cases, 35.90%) in group III. This suggests that, despite increased activity levels in early childhood (group I) during the growth period, the lower extremities may be less developed, leading to a higher propensity for slipping. It can be inferred that the period encompassing kindergarten and the early years of primary school is marked by a significant increase in activity, while there may be less parental supervision than during the initial growth period.
In the pediatric population, accidents related to sports or social activities were observed exclusively within school-age groups, except for one case in group I. Assault injuries were also confined to school-age groups, with one case occurring in the lower grades and two cases in the upper grades of primary school. These findings suggest that social activities, including sports, are more common among school-age children than among those under the age of 6, and that incidents of assault begin to emerge within this age group.
Fourth, it has been reported that the incidence of frontal impact (FI) fractures is significantly higher in preschool and elementary school-aged children than in adolescents and adults, in contrast to lateral impact (LI) fractures [4]. In this study, group I experienced nine cases of FI fractures, 14 cases of LI fractures, and one case of frontal impact plane II (FII) fractures. Group II had 14 FI fractures, 19 LI fractures, and two FII fractures. Group III contained 13 FI fractures, 19 LI fractures, two FII fractures, and five cases of lateral force plane II (LII) fractures. These results show that type I fractures were present in 89.8% of cases, including 41 fractures from FI and 57 from LI. These findings imply that pediatric nasal fractures are typically minor and occur with similar frequency regardless of the child’s age. Additionally, there was no significant difference in the injury vectors between frontal and lateral forces.
Fifth, the incidence of concurrent septal fractures in cases of nasal bone fractures across all age groups has been reported to be 46.9% and 47.4% [13,14]. Septal injuries in pediatric patients with nasal fractures are of particular concern because they may impair facial growth by disrupting a growth center [15]. However, it remains uncertain whether a nasal bone fracture alone could contribute to septal deviation in adults, even in the absence of a septal fracture [16].
In this study, the overall number of septal injuries in patients with pediatric nasal fractures was 14 (14.29%). There was one patient with a septal injury out of 24 patients (4.17%) in group I, as well as two of 35 patients (5.71%) in group II and 11 of 39 patients (28.21%) in group III. These results suggest that the risk of septal injury is relatively low during the first growth period. However, there is a statistically significant increase in risk as children advance to the higher grades of primary school (p< 0.05). Notably, the incidence of septal injuries in uppergrade students was nearly five times greater than that in children attending kindergarten and the lower grades of primary school (Fig. 1).
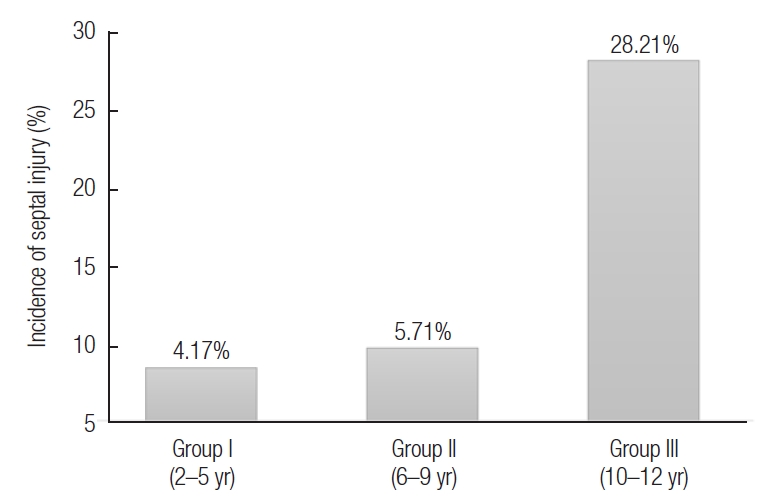
Incidence of septal injuries by age group. There was one patient with septal injury out of 24 patients (4.17%) in group I, as well as two of 35 patients (5.71%) in group II, and 11 of 39 patients (28.21%) in group III. The probability of septal injury increased with age, and the prevalence of septal injuries in the upper grades was about five times higher than that in the lower grades of primary school.
Although this study identified clear differences in nasal bone fractures among pediatric patients across various age groups, limitation is that the findings are based solely on patients who underwent surgical treatment. To achieve a more comprehensive understanding of this condition, further research that includes patients who received conservative treatment is necessary. Additionally, pediatric nasal fractures pose challenges due to injuries to the cartilage framework, which often lead to secondary nasal deformities and a higher risk of long-term functional or external nasal issues, even with accurate diagnosis and optimal treatment [17,18]. Therefore, it is essential to assess objective outcomes during long-term follow-up, categorized by age group.
The present study compared clinical characteristics of nasal bone fractures during early childhood, later childhood, and the growth period of the nose, taking into account differences in developmental environments and the impact of growth spurts. This comparison may offer valuable insights into the nature of pediatric nasal bone fractures.
Notes
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Funding
None.
Ethical approval
The study was approved by the Institutional Review Board of Daegu Catholic University Medical Center (IRB No. CR-23-057-L) and performed in accordance with the principles of the Declaration of Helsinki. The informed consent was waived.
Author contributions
Conceptualization; Data curation; Formal analysis: Dong Gil Han. Methodology; Project administration: Jun Woo Kim, Dong Gil Han. Visualization: Jun Woo Kim. Writing - original draft: Jun Woo Kim, Dong Gil Han. Writing - review & editing: Jun Woo Kim, Dong Gil Han. Investigation: Jun Woo Kim, Dong Gil Han. Resources; Software: Jun Woo Kim. Supervision; Validation: Dong Gil Han.
Abbreviations
FI
frontal impact
FII
frontal impact plane II
LI
lateral impact
LII
lateral force plane II