Periantral fungal abscess after zygoma reduction: a case report
Article information

Abstract
This case report describes our treatment of a persistent periantral abscess in a 35-year-old woman. The abscess developed following a zygoma-reduction surgery, during which a preexisting fungal ball had not been addressed. Our comprehensive treatment approach included functional endoscopic sinus surgery, fungal ball removal, abscess drainage, and debridement. Two weeks postoperatively, the patient’s symptoms had resolved. A 6-month postoperative follow-up revealed no signs of recurrence or complications, and the patient reported satisfactory functional and aesthetic results. This case underscores the importance of thorough preoperative evaluations and raises awareness about the potential risks of untreated asymptomatic pathologies, which can potentially progress and lead to further complications.
INTRODUCTION
A fungal ball is a type of noninvasive fungal sinusitis that primarily occurs in the maxillary sinus; it is more common in women than in men, and it usually presents unilaterally [1]. The pathophysiology of asymptomatic fungal balls is not clearly understood, but they typically affect patients who do not have risk factors related to immunosuppression [2]. Asymptomatic cases generally do not require surgical interventions. However, fungal balls are occasionally identified and treated incidentally during tests conducted to detect infection before initiating immunosuppressive therapy or implant surgery [3]. Before zygoma-reduction surgery, imaging studies are conducted to facilitate the planning of the surgery and to identify any pathology within the sinus. It is recommended to treat all pathologies prior to implant insertion [4]. Herein, we present our experience of treating a patient with a fungal ball that was not identified or treated prior to zygoma-reduction surgery. The untreated fungal ball subsequently led to periantral soft-tissue invasion.
CASE REPORT
A 35-year-old woman presented at our hospital with a persistent left periantral abscess, which had developed after she underwent zygoma-reduction surgery at a local clinic. She had twice undergone incision and drainage through the gingivobuccal sulcus, and methicillin-resistant Staphylococcus aureus (MRSA) had been identified in the culture taken at the local clinic where she had undergone malarplasty. Vancomycin was administered, but no improvement had been observed. Therefore, she was subsequently transferred to our hospital. On arrival, she was febrile and complained of nasal stuffiness, which had not been present prior to the malarplasty. We also noted a persistent soft-tissue abscess, characterized by erythematous swelling, crepitus, and fluctuation on her left side (Fig. 1).
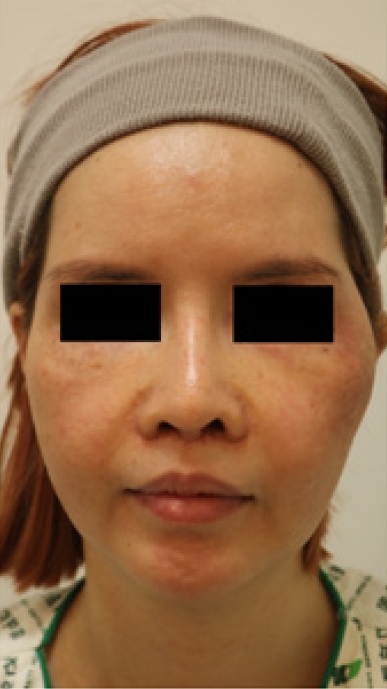
A 35-year-old woman with persistent swelling, redness, and pain in the left facial area following malarplasty.
The patient’s immune status was investigated. A complete blood count and HIV test results showed no abnormalities. Furthermore, we found no medical records or test results indicating the use of immunosuppressive agents or any cancer treatment.
A computed tomography (CT) scan revealed a lesion in the left maxillary sinus. This lesion had a density consistent with that of soft tissue and contained calcific deposits (Fig. 2). An abscess was also confirmed in the soft tissue surrounding the left temple and zygoma. CT and panoramic radiography revealed no odontogenic origins.
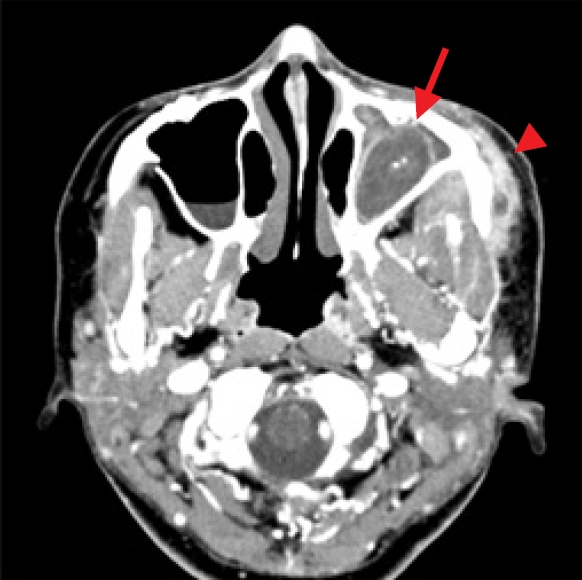
Preoperative computed tomography showing an abnormal area of density similar to that of soft tissue and calcific deposits inside the left maxillary sinus, suggestive of a fungal ball (arrow). Subperiosteal abscess formation is suspected around the zygoma (arrowhead).
Upon reviewing the patient’s medical history, including prior CT findings before the malarplasty (Fig. 3) and information from her medical records, it was determined that she had developed a periantral abscess following the malarplasty, in the context of an existing fungal ball.
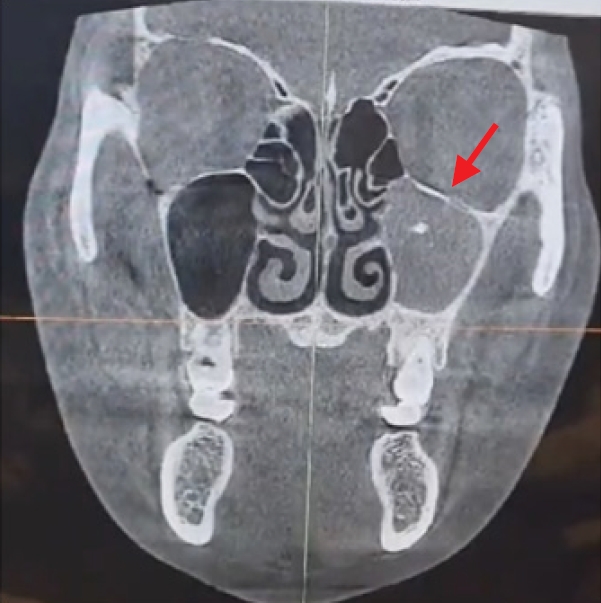
Computed tomography taken for planning purposes at a local plastic surgery clinic prior to zygoma reduction. Evidence of suspected noninvasive fungal sinusitis can be observed in the left maxillary sinus (arrow).
In collaboration with an otorhinolaryngologist, we performed functional endoscopic sinus surgery (FESS) and a middle meatal antrostomy to fully extract the fungal ball from the sinus. A postoperative tissue examination revealed the presence of Aspergillus hyphae (Fig. 4). Simultaneously, we accessed the maxilla through an intraoral incision and completely drained the abscess. In the area where the malarplasty had been performed, we conducted additional debridement around the plate and bone. There were no signs of maxillary bone malabsorption or loosening of the titanium plate and screws from the prior malarplasty. Therefore, we decided not to proceed with plate replacement. Once the bleeding was controlled, the incision site was closed without additional drain insertion.

A microscopic image of a fungal ball stained with Gomori methenamine silver (×200). A typical sign of Aspergillus hyphae was observed, as shown by grayish-black staining, with branches at acute angles and showing septation between the hyphae.
Approximately 2 weeks postoperatively, antibiotics were discontinued after the swelling, redness, and hardening of the facial skin subsided. A follow-up CT scan revealed a reduction in the extent of the abscess and sinusitis (Fig. 5).
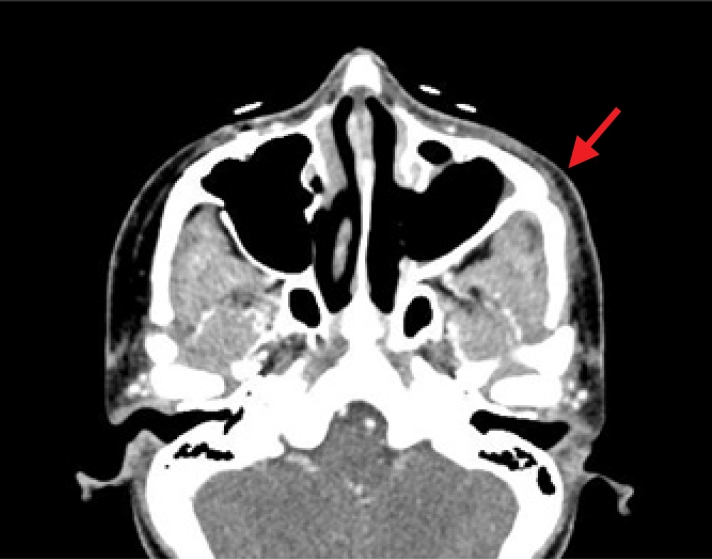
Computed tomography at 2 months following final debridement (arrow). Improvement in the signs of infection around the left maxillary sinus and left zygoma can be observed.
At 6 months postoperatively, there were no signs of recurrence or suspicious findings suggestive of complications, such as a fistula due to nonunion of the bone, malocclusion, or sinking of the malar area. The patient expressed satisfaction with both the functional and aesthetic outcomes (Fig. 6A). Furthermore, an endoscopic examination revealed no remaining signs of inflammation in the maxillary sinus mucosa (Fig. 6B).

(A) At 6 months after debridement, all signs of infection have fully resolved. (B) The maxillary sinus shows complete mucosal recovery on nasal endoscopy, indicating a good outcome.
DISCUSSION
Generally, sinusitis should be treated before malarplasty, because the procedure can potentially worsen the infection, delay postoperative healing, or lead to nonunion [5]. As a result of this common practice, complications arising from malarplasty in patients with sinusitis are relatively rare. Moreover, no cases have been documented in which malarplasty was performed in a patient with a fungal ball, a condition that is much less common than sinusitis.
Noninvasive fungal balls can develop in patients who show no signs of being immunocompromised and are often misdiagnosed [6]. In this patient, a preoperative CT scan had been conducted to prepare for malarplasty. Although the scan had revealed suspicious findings indicative of a fungal ball, including peripheral bony erosion in the high-density areas within the sinus, the fungal ball had not been initially diagnosed. This oversight subsequently resulted in postoperative complications (Fig. 3) [7].
The detection of MRSA in the postoperative facial abscess raised questions concerning the origin of the abscess. One possibility is that the abscess developed from an invasive form of the preexisting fungal ball. Alternatively, external pathogens introduced during surgery or other factors, such as a hematoma, may have contributed to abscess formation.
The surgical findings and facial CT scans showed a noticeable connection between the sinus and the abscess at the osteotomy site. This evidence suggests that the facial abscess had developed subperiosteally. Furthermore, we observed Aspergillus hyphae in the sample taken from the facial abscess.
Endoscopic procedures, such as noninvasive FESS, are widely used to treat fungal balls, and their effectiveness has been welldocumented in previous reports [3,8]. In this patient, we improved the ventilation of the obstructed maxillary ostium by removing the uncinate process. We then performed a middle meatal antrostomy using FESS to eradicate the fungal ball completely. It has been reported that a facial abscess surrounding a titanium plate must be entirely removed to eliminate the infection source [5]. However, given the diminished adsorption and biofilm formation ability of S. aureus on titanium [9], and the lack of reports linking titanium to pathological sinus disease [10], we performed subperiosteal dissection through an intraoral approach. This procedure exposed the layer containing the abscess, which was then drained [11]. Following this, we debrided the area surrounding the prosthesis after drainage to the maximum extent possible.
At 6 months postoperatively, no signs of facial abscess recurrence were observed. Furthermore, the patient did not exhibit any complications, such as malocclusion, fistula, or alterations in facial contour, and the patient expressed satisfaction with the outcome.
Although fungal balls are uncommon, asymptomatic patients with this condition are at risk of progressing to invasive fungal sinusitis over time, potentially leading to fatal outcomes [12]. This risk can be heightened by surgical procedures involving the sinus wall. Therefore, careful observation is crucial prior to sinus surgery, such as malarplasty, both during the preoperative surgical planning stage and when inspecting for abnormal inflammation or infections at the surgical site. Complications can be mitigated through targeted preoperative evaluations and treatment.
Notes
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Funding
None.
Ethical approval
The report was approved by the Institutional Review Board of Konyang University Hospital (IRB No. 2023-06-014).
Patient consent
Written informed consent was obtained from the patient to use and publish her images.
Author contributions
Conceptualization: In Chang Koh. Data curation; Formal analysis: Keun Hyung Kim. Methodology; Project administration; Visualization: In Chang Koh. Writing - original draft: Keun Hyung Kim. Writing - review & editing: In Chang Koh. Investigation: Keun Hyung Kim. Resources: Keun Hyung Kim. Software: Keun Hyung Kim. Supervision: Hoon Kim, Soo Yeon Lim. Validation: Soo Yeon Lim, In Chang Koh.
Abbreviations
CT
computed tomography
FESS
functional endoscopic sinus surgery
MRSA
methicillin-resistant Staphylococcus aureus