Comparison of pain relief in soft tissue tumor excision: anesthetic injection using an automatic digital injector versus conventional injection
Article information

Abstract
Background
The pain caused by local anesthetic injection can lead to patient anxiety prior to surgery, potentially necessitating sedation or general anesthesia during the excision procedure. In this study, we aim to compare the pain relief efficacy and safety of using a digital automatic anesthetic injector for local anesthesia.
Methods
Thirty-three patients undergoing excision of a benign soft tissue tumor under local anesthesia were prospectively enrolled from September 2021 to February 2022. A single-blind, randomized controlled study was conducted. Patients were divided into two groups by randomization: the experimental group with digital automatic anesthetic injector method (I-JECT group) and the control group with conventional injection method. Before surgery, the Amsterdam preoperative anxiety information scale was used to measure the patients’ anxiety. After local anesthetic was administered, the Numeric Pain Rating Scale was used to measure the pain. The amount of anesthetic used was divided by the surface area of the lesion was recorded.
Results
Seventeen were assigned to the conventional group and 16 to the I-JECT group. The mean Numeric Pain Rating Scale was 1.75 in the I-JECT group and 3.82 in conventional group. The injection pain was lower in the I-JECT group (p< 0.01). The mean Amsterdam preoperative anxiety information scale was 11.00 in the I-JECT group and 9.65 in conventional group. Patient’s anxiety did not correlate to injection pain regardless of the method of injection (p= 0.47). The amount of local anesthetic used per 1 cm 2 of tumor surface area was 0.74 mL/cm2 in the I-JECT group and 2.31 mL/cm2 in the conventional group. The normalization amount of local anesthetic was less in the I-JECT group (p< 0.01). There was no difference in the incidence of complications.
Conclusion
The use of a digital automatic anesthetic injector has shown to reduce pain and the amount of local anesthetics without complication.
INTRODUCTION
Pain is defined as the perceived sensory and emotional reaction to actual or perceived tissue injury by the International Association for the Study of Pain [1]. Pain caused by local anesthetic injection makes patients anxious before surgery. It results in sedation or general anesthesia during excision surgery which could be performed with just local anesthesia. Avoiding sedation or general anesthesia could reduce costs, time, and side effects such as nausea, vomiting, cardiorespiratory compromise, and urinary retention [2]. Perception of pain varies from individual to individual. This is because pain can be exaggerated in connection with various factors such as past experiences, stress, and anxiety [3].
Pain during injection of local anesthetic is caused due to the skin piercing of the needle or the pressure of the solution stretching the skin [4]. This injection pain could be reduced by several methods such as using more than one type of sensory noise, inserting the needle perpendicularly, using smaller needle, or slowing the rate of injection [4,5].
Since the density or resistance of tissues varies from person to person and for each body part, it is difficult to control the pressure and injection speed in the method of injecting local anesthesia by pushing the piston of a syringe by operator’s hand. However, computer-controlled local anesthetic delivery system could deliver local anesthesia at a constant rate and volume regardless of the density or resistance of tissues [6].
In this study, we compared pain during local anesthesia using conventional methods with dental syringe to digital automatic anesthetic injectors.
METHODS
This single-blind, randomized controlled study was conducted from September 2021 to February 2022. All patients undergoing excision under local anesthesia were eligible for this study. Exclusion criteria included the need for sedation or the presence of signs of infection. Written informed consent was obtained from all patients. Patients were divided into two groups by randomization: the experimental group with digital automatic anesthetic injector method and the control group with conventional injection method. Local anesthetics were used in both groups with a mixture of 2% lidocaine and 1:100,000 epinephrine (Huons). The conventional method utilized a dental anesthetic syringe (Osung MND) with a 30-gauge needle for local anesthesia, while the experimental group used digital automatic anesthetic injector, I-JECT (Medihub), with a 30-gauge needle for local anesthesia. The injector incorporates a button-controlled mechanism for tuning the injection rate of the mixture across four stages. Users can select their preferred mode to alter the mixture’s injection speed (P mode: 1.8 mL/465 sec, mode 1: 1.8 mL/202 sec, mode 2: 1.8 mL/125 sec, mode 3: 1.8 mL/47 sec). In this study, the mixture was injected at the pace associated with mode 2.
The demographic and clinical data including age, smoking history, and medical history (e.g., diabetes mellitus, hypertension), were investigated in all patients during the outpatient clinic. Before surgery, the Amsterdam Preoperative Anxiety and Information Scale (APAIS) was used to measure the patients’ anxiety regarding local anesthesia and surgery. APAIS consists of six questions, each of which can be scored from 1 to 5. In this study, only the four questions related to anxiety were used, and the patient’s preoperative anxiety level was evaluated on a scale of 4 to 20. After local anesthesia was administered, the Numeric Pain Rating Scale (NPRS) was used to measure the pain of the anesthesia injection. Patients measure the intensity of pain by selecting a number from 0 to 10, with higher numbers indicating more severe pain. It was confirmed whether there were any side effects, such as bleeding or bruising, at the injection site. The amount of anesthetic used after surgery was recorded. The amount of anesthetic used was divided by the surface area of the lesion to calculate the amount of anesthetic used per unit area, making it possible to compare it by standardizing. The pain at the surgical site was measured using the NPRS during the first outpatient visit after the surgery. The presence of side effects such as hematoma, seroma was also checked. All surgical procedures, including local anesthesia, were performed by the same plastic surgeon. Local anesthetics were injected along the boundary of the tumor. We tried to reduce the pain through sensory noise by tapping around the tumor. Except for the method of anesthesia, the surgical procedure, dressing, and postoperative management were carried out in the same manner as usual. IBM SPSS version 21.0 (IBM Corp.) was used to analyze the results. Representative data were presented as the mean ± standard deviation. The chi-square or Fisher exact test was used for categorical data, and the Student t-test or Mann-Whitney U-test was used for continuous data. p-values below 0.05 were applied as the cutoff for statistical significance.
RESULTS
Thirty-three patients were evaluated in this study and there were no dropouts. Using a random number generator to classify patients, 17 were assigned to the conventional method group and 16 were assigned to the I-JECT group. Table 1 shows the demographic characteristics. There was no significant difference in demographics and past medical history such as hypertension, diabetes mellitus, and heart disease between the two groups. The operation sites were divided into three areas: head and neck, trunk, and extremities, and the proportion of each site did not show a statistically significant difference.

Demographics and location of the mass
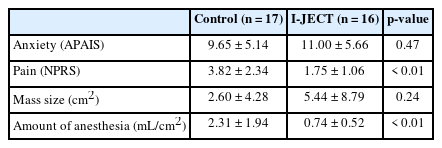
Table 2 compares the outcomes between the conventional group and the I-JECT group. The degree of anxiety about local anesthesia and surgery, as evaluated by APAIS, was higher in the I-JECT group (11.00 ± 5.66) than in conventional group (9.65 ± 5.14), but there was no statistical difference between the two groups (p = 0.47). The NPRS for pain experienced during local anesthetics injection was lower in the I-JECT group (1.75 ± 1.06) than in conventional group (3.82 ± 2.34), showing a statistically significant difference (p < 0.01). The size of the mass did not show statistically significant differences between the conventional (2.60 ± 4.28 cm2) and the I-JECT groups (5.44 ± 8.79 cm2) (p = 0.24). The amount of local anesthetic used per 1 cm 2 of tumor surface area was lower in the I-JECT group (0.74 ± 0.52 mL/cm2) compared to the conventional group (2.31 ± 1.94 mL/cm2) (p < 0.01). There was no statistically significant difference in side effects and pain felt by patients at the surgical site, and no correlation was found between APAIS and pain intensity.
Comparison of outcomes between control group and IJECT group
Table 3 shows the pathological type of the masses. There was no significant difference in the pathological type of the mass between the two groups (p = 0.36).

Comparison of pathological types of mass
DISCUSSION
This study was a randomized controlled single-blind study comparing pain during local anesthesia using conventional methods with dental syringe and digital automatic anesthetic injectors measured by the NPRS. Computer-controlled local anesthetic delivery is used in dental surgery to reduce patient pain during local anesthesia, and several studies prove its advantages [7-9]. However, their stability has not yet been established in plastic surgery, which frequently uses local anesthesia. This study is important as it is a prospective study that verifies the safety and efficacy of a digital automatic anesthetic injector in plastic surgery.
Pain is a complex and subjective sensation that is influenced by various factors as patients can experience varying degrees and forms of pain [1,3]. There are various techniques that can help alleviate the discomfort caused by injection pain, including the utilization of multiple forms of sensory noise, administering the needle perpendicularly, opting for a smaller needle, or gradually decreasing the injection rate [4,5,10]. However, previous attempts have focused on changing the technique and we have tried to change the tools used for anesthesia.
The digital automatic anesthetic injector can inject local anesthesia with constant pressure and speed, regardless of the tissue density or resistance [9]. It also has the advantage of maintaining a consistent performance, independent of the operator’s fatigue or skill level. This injector costs approximately 1.6 million Korean won, but it can be used multiple times by simply replacing the needle. When anesthesia is first injected, a high pressure needs to be quickly injected to overcome tissue resistance, causing severe pain to patients. If the anesthesia is injected slowly, the tissue will expand slowly, reducing the pain [5], but the total time required for anesthesia may increase, potentially leading to an increase in pain perceived by the patient.
NPRS is an effective and valid tool for measuring pain in many areas [11], including excision surgery. In this study, the pain felt by patients under local anesthesia was 3.85 on average in the conventional group and 1.75 in the I-JECT group. This is consistent with a study that compares the pain felt by patients using conventional methods and a digital automatic anesthetic injector during local anesthesia in dental surgery.
In plastic surgery, excision of benign tumors can be performed with local anesthesia if the depth of the tumor is not deeper than the muscle layer or the size is not very large. However, there may be cases where surgery is delayed due to concerns about the pain that occurs with local anesthesia, resulting in tumor growth, or unnecessary sedation or general anesthesia is performed because the situation becomes worse and local anesthesia is no longer possible. Especially in old age, skin cancer is commonly found, and it can be adequately excised and reconstruction with local anesthesia [12,13]. However, if general anesthesia is performed due to fear of local anesthesia, patients may experience complications such as atelectasis, arrhythmia, renal complications, and even death [14]. Therefore, based on the results of this study that the use of a digital automatic anesthetic injector can reduce pain felt by patients during local anesthesia, it is expected that the frequency of sedation or general anesthesia performed due to patient anxiety over pain during excision surgery performed under local anesthesia can be reduced.
The administration of epinephrine can cause skin necrosis because of its vasoconstrictive properties and lidocaine can cause severe side effects such as arrhythmia, blindness, and shock [15-19]. Consequently, reducing the amount of the mixture of 2% lidocaine and 1:100,000 epinephrine can lower the potential for the adverse effects outlined previously. In this study, the results showed that using a digital automatic anesthetic injector could reduce the amount of local anesthetics used. Additionally, this machine can perform aspiration to confirm whether the needle has not been inserted into the vessel. It is expected that this will allow patients to receive surgery in a safer environment.
In general, it is known that there is a correlation between the level of anxiety that patients feel before surgery and the amount of pain they experience during surgery [3]. APAIS score is widely used in studies that evaluate anxiety, as it is a score used to evaluate patients’ anxiety before surgery [20]. In this study, by showing that there was no difference in anxiety as evaluated by APAIS between the conventional group and the experimental group, we were able to reduce bias caused by this.
Moreover, different depths of mass or different parts of the body have different sensitivities to pain, which can cause bias. In this study, the depth of the mass in both groups was the same at the skin or subcutaneous level, and the pathologic type of the mass did not show statistically significant difference. The study demonstrated that there was no difference in the distribution of surgical locations between the conventional and I-JECT groups, reducing possible bias in this regard.
With conventional methods, the operator’s sensory feedback during the injection process allows them to adjust the speed and direction of the injection to minimize pain. I-JECT can also adjust the direction during the injection process and adjust the injection speed, but since the injection speed can only be adjusted in four stages, it is not as free as the conventional method. Although the I-JECT is reusable, it has the disadvantage of being more expensive than a dental syringe, and the electronic nature of the device requires regular maintenance. In addition, there is a risk of overdosing on local anesthetic in the event of malfunctions or technical failures.
In conclusion, this study highlights the effectiveness and safety of digital automated anesthesia injectors in relieving pain during local anesthesia. The device was found to provide superior pain relief compared to conventional methods, reducing the amount of local anesthetic required. The findings suggest that the use of a digital auto-injector can increase patient comfort and potentially reduce the need for sedation or general anesthesia.
Notes
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Funding
This Research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (Grant number: HI16C2319).
Ethical approval
The study was approved by the Institutional Review Board of Gachon Gil Medical Center (IRB No. GCIRB2021-326) and performed in accordance with the principles of the Declaration of Helsinki. Written informed consent was obtained from all patients.
Author contributions
Conceptualization: Yu Jin Kim. Data curation: Hye Gwang Mun, Bo Min Moon. Formal analysis: Hye Gwang Mun. Funding acquisition; Project administration: Yu Jin Kim. Visualization; Writing - original draft: Hye Gwang Mun. Writing - review & editing: Hye Gwang Mun, Yu Jin Kim. Investigation: Hye Gwang Mun, Bo Min Moon, Yu Jin Kim. Software: Hye Gwang Mun. Supervision: Yu Jin Kim.
Abbreviations
APAIS
Amsterdam Preoperative Anxiety and Information Scale
NPRS
Numeric Pain Rating Scale