The effect of the dental root on single mandibular bone fractures
Article information
Abstract
Background
This study was conducted to determine the effect of the distributional relationship between dental roots and the mandibular bone on single mandibular bone fractures, which are common craniofacial fractures.
Methods
This was a retrospective, single-center study in Seoul, Korea. Patients with single mandibular fractures in the symphysis, parasymphysis, body, and angle area, with tooth structure involvement were included. The control group included patients with simple, bone-level lacerations without fractures. In total, 94 patients (72 males and 22 females) were included in the treatment group, and 125 (71 males and 54 females) were included in the control group. The height of the mandibular bone and the dental root were measured with panoramic radiography. The central incisor represented the symphysis area, the canine represented the parasymphysis area, the first molar represented the body area, and the second molar represented the angle area.
Results
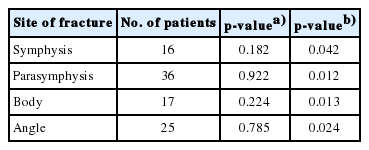
In the treatment group, symphysis fractures occurred in 16 patients (17%), parasymphysis fractures in 36 patients (38%), body fractures in 17 patients (18%), and angle fractures in 25 patients (27%). The ratios of the dental roots to the total height of the mandibular bone in the treatment group were 30.35%, 39.75%, 39.53%, and 36.27% for symphysis, parasymphysis, body, and angle areas, respectively, whereas in the control group, they were 27.73%, 39.70%, 36.76%, and 35.48%. The ratios of the treatment group were significantly higher than those of the control group.
Conclusion
The results show that the higher ratio of the dental root to the height of the mandibular bone increases the fracture risk.
INTRODUCTION
Mandibular fractures are common among fractures of the craniofacial region [1,2]. Approximately 20% to 80% of patients with maxillofacial fractures have been reported to have mandibular fractures in previous studies [1-4]. Although both pathologic and traumatic events may induce fractures in the mandibular region, trauma is the main cause [5]. Traumatic mandibular fractures are classified into several anatomical groups according to the fracture sites: symphysis, parasymphysis, body, angle, subcondyle, condyle, and ramus [2,6]. Among these areas, the sites that have structural relationships with the teeth are the symphysis, parasymphysis, body, and angle areas. Zhou et al. [7] reported the pattern of dental injury distribution in mandibular fractures, and other studies have also been conducted on the relationships between maxillofacial fractures and the types or occurrence of dental injuries [1,8]. However, a literature review yielded no studies on the relationships between the roots of the teeth and the mandibular bone in association with mandibular bone fractures. Accordingly, in this study, we aimed to determine the effect of the distributional relationships between the dental roots and their locations in the mandible on mandibular bone fractures.
METHODS
The protocol, survey, and consent forms were reviewed and approved by the Institutional Review Board of Konkuk University Medical Center (IRB No. KUH1280115). We reviewed a total of 203 patients with isolated single mandibular fractures who were treated in the Department of Plastic and Reconstructive Surgery, with complete medical records from February 2008 to September 2017. This study was performed retrospectively in a single center. Patients with multiple fracture sites, those with dental injuries, and those with third molars were excluded from the study.
Only traumatic fractures were included in the treatment group and, to limit the traumatic area, only patients with bone-level lacerations in the mental area were included in the treatment group. The total number of the patients who fulfilled the inclusion criteria was 94. The control group included patients with simple, bone-level lacerations without fractures.
For comparative analysis, a total of 125 patients with bonelevel lacerations in the mental area were included as a control group. As shown in Fig. 1, height of the mandibular body (a), length of the tooth root (b), height of the mandibular bone excluding the length of the tooth root (c), was defined.
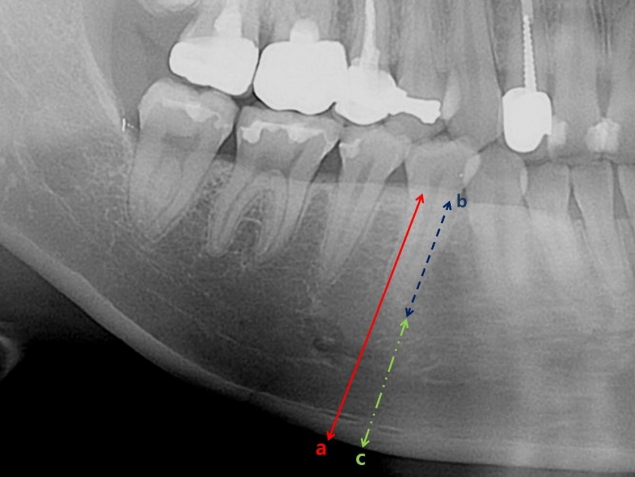
The mandibular body area: (a) height of the mandibular body (red solid line), (b) length of the tooth root (blue dashed line), (c) height of the mandibular bone excluding the length of the tooth root (a–b, green dashed-dotted line).
We also defined the mandibular bone fractures in the treatment group according to fractures in the mandibular symphysis, parasymphysis, body, and angle areas. The central incisor, canine, first molar, and second molar were adopted as representative teeth for the aforementioned mandibular areas, respectively. We analyzed panoramic radiographs with viewer software (Centricity PACS, Radiology RA1000 Workstation; GE Healthcare, Boston, MA, USA) to measure the length of the dental roots and the mandibular bone in each area for all of the included patients. Using these measurements, we calculated and compared the ratios of the height of the mandibular bone excluding the dental root to the dental root, and assessed ratio of the root length to the mandibular height (100×b/a).
Nonparametric analysis of the treatment and control groups was performed. To compare the two groups, we used two-sampled Wilcoxon rank-sum (Mann-Whitney) test to rank the differences in the average values of each of the four fractures sites in the treatment and control groups, using STATA ver. 14.0 (STATACorp., College Station, TX, USA).
RESULTS
Age and sex
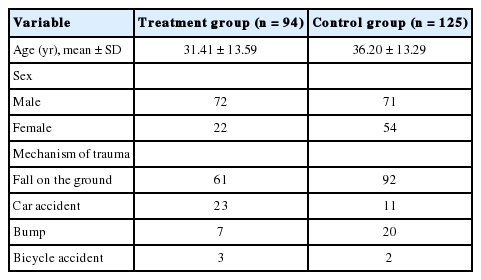
The treatment group included 72 male and 22 female patients. Regarding the fracture sites, 16 patients (12 males, four females) comprised the symphysis area group, 36 patients (25 males, 11 females) comprised the parasymphysis area group, 17 patients (15 males, two females) comprised the body area group, and 25 patients (20 males, five females) comprised the angle area group. The control group included 71 male and 54 female patients. The ratio of male to female patients was 3.27:1 in the fracture group and 1.31:1 in the control group. The average age (±standard deviation [SD]) was 31.41 (±13.59) years in the treatment group and 36.20 (±13.29) years in the control group (Table 1).
Patient characteristics
Mechanism of trauma
The most common cause of fractures was trauma to the mandible resulting from falling to the floor, the causes of which included syncope, stumbling on an object, and falling during exercise. Both blackout and non-blackout cases were included. The second most common cause was traffic accidents in the treatment group and crashing into objects without falling to the floor (i.e., violence, being hit by an object) in the control group (Table 1).
Ratio of the height of the mandibular bone excluding the dental root to the dental root
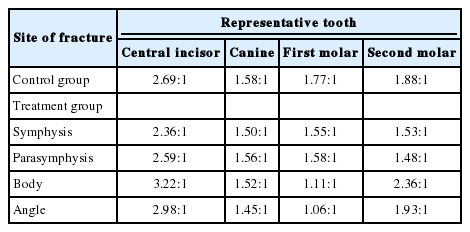
We calculated the ratio of the height of the mandibular bone excluding the dental root to the dental root in the four mandibular areas. In the symphysis fracture group, the ratio of to the central incisor root was 2.36:1. The ratio was 1.56:1 for the canine root in the parasymphysis fracture group, 1.11:1 for the first molar root in the body fracture group, and 1.93:1 for the second molar root in the angle fracture group (patients with third molars were excluded from the study). In the control group, the ratios of the mandibular bone to the dental root were 2.69:1, 1.58:1, 1.77:1, and 1.88:1, respectively, at the four area previously mentioned in the fracture group (Table 2).
The ratio of the height of the mandibular bone excluding the dental root to the dental root in the group
As a result of the two-sampled Wilcoxon rank-sum (Mann-Whitney) test for each site between the treatment and control groups, the p-values of the symphysis, parasymphysis, body, and angle areas were 0.182, 0.922, 0.224, and 0.785, indicating no significant result in the entire area (Table 3).
Wilcoxon rank-sum (Mann-Whitney) test
Ratio of the root length to the mandibular height
Next, we compared the ratio of the root length to the mandibular height (100×b/a) at the four sites. In the control group, the percentile values (±SD) of the data were 27.73% (±4.31%) for the central incisor root in the symphysis area, 39.70% (±6.39%) for the canine root in the parasymphysis area, 36.76% (±5.75%) for the first molar root in the body area, and 35.48% (±5.40%) for the second molar root in the angle area (Table 4). In the treatment group, as a result of the same calculations, the final values were 30.35% (±4.68%) in the symphysis area, 39.75% (±5.48%) in the parasymphysis area, 39.53% (±4.32%) in the body area, and 36.27% (±9.28%) in the angle area, respectively (Table 4).
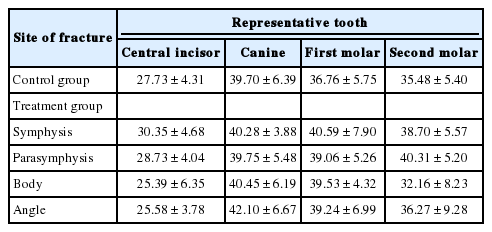
The ratio of the root length to the mandibular height (100×b/a) in the group (%)
As a result of the two-sampled Wilcoxon rank-sum (Mann-Whitney) test for each site between the treatment and control groups, the p-values of the symphysis, parasymphysis, body, and angle areas were 0.042, 0.012, 0.013, and 0.024, respectively, and all of the results were statistically significant (Table 3).
DISCUSSION
Among the facial bones, the mandible is the only mobile part, and in addition, it is prone to fractures [1,4]. Although it is difficult to clearly understand the correlations between dental structures and mandibular structures in mandibular bone fractures, several studies have been conducted on this issue. Duan and Zhang [9] reported that the presence of a third molar in the mandible increases the risk of mandibular angle fracture and simultaneously reduces the risk of condylar fracture. They considered whether patients had third molars, but did not address the relationship between the dental root and mandibular structures according to their proportional correlations.
Another study reported the correlations between dental injuries and mandibular fractures [4]. As in our study, isolated single mandibular fractures were analyzed and dental injuries of the lower-anterior teeth were found to be significantly more common in the symphysis area. Lower-posterior dental injuries were significantly more common in body and angle fractures, indicating a major correlation between dental injuries and mandibular fracture sites. However, no studies on isolated single fractures without dental injuries were found in the literature and, therefore, we could not determine specific interactions between isolated single fracture sites and dental structures.
Thoren et al. [8] studied the relationships of dental injuries and maxillofacial fractures, reporting that fractures were most common around the incisor region in both maxillary and mandibular areas. This was also similar to the findings of our study; we observed that parasymphysis fractures were the most common, at 38.20%. Additionally, ratio of the root length to the mandibular height showed statistically significant results (p<0.05) in the incisor region, which has been thoroughly explained in previous studies.
We assessed patients based on two points: the ratio of the height of the mandibular bone excluding the dental root to the dental root, and ratio of the root length to the mandibular height. In our assessment results, the ratios of height of the mandibular bone excluding the length of the tooth root to length of the tooth root themselves were nonsignificant. However, the ratio of (100×b/a) differed significantly in all four anatomical areas compared to the control group (p<0.05) (Table 3). On the basis of the results, it is concluded that the risk of fracture is higher when the ratio of (100×b/a) is higher even in the similar circumstances of traumatic force. This is crucial because no previous research has been conducted on the correlations between the height of the mandible and the dental root in isolated single mandibular fractures.
Our study had several limitations. This research was retrospective, access was limited to registered medical records, and sample size was relatively small. In cases of angle fractures, interactive effects of third molars could not be explained because patients with third molars were not included in the study. Additionally, correlational effects of the structures in multiple mandibular fractures were not reviewed in the study.
Notes
No potential conflict of interest relevant to this article was reported.
PATIENT CONSENT
The patients provided written informed consent for the publication and the use of their images.