Reconstruction of temporal hollowing deformities using silicone implants made using a toy-clay model: a report of three cases
Article information

Abstract
Severe temporal hollowing deformities can occur in patients who undergo craniectomy after intracranial hemorrhage. Reconstruction surgery for cosmetic purposes using silicone implants in patients with temporal hollowing deformities after craniectomy is advantageous because the procedure is simple and rapid, with a short recovery time, resulting in lower overall treatment costs. Of paramount importance, this option yields highly satisfactory results for patients. The authors present three cases of simple and fast surgery using silicone implants where highly satisfactory outcomes were obtained.
INTRODUCTION
In cases of intracranial hemorrhage, decompressive craniectomy is performed to reduce the intracranial pressure by removing a section of the skull, thereby allowing the enlarged cerebral ventricles to expand without compression [1,2]. Studies have reported that removing larger pieces of calvarial bone results in a greater decrease in intracranial pressure [3]. Once the patient recovers sufficiently after craniectomy, the removed portion needs to be reconstructed for brain protection. If possible, the original skull piece should be preserved until the patient recovers and then used to close the defect via cranioplasty [4]. However, if the preserved bone graft cannot be used or the surrounding soft tissue is extensively damaged, a severe hollowing deformity may develop.
Various methods exist for the surgical reconstruction of cranial hollowing deformities that result from craniectomy. The most traditional method is autologous reconstruction using rib or split calvarial bone graft. Alloplastic reconstruction has recently emerged as a widely accepted treatment option. In 2009, Hanasono et al. [5] introduced a skull reconstruction method using polyetheretherketone implants. In 2012, Lin et al. [6] reported a method using porous polyethylene implants for skull reconstruction in children. In 2015, Cho et al. [7] introduced a surgical method to reconstruct the skull with a custom-made three-dimensional titanium implant. In 2018, Kim et al. [8] used an autologous calvarial onlay graft to prevent temporal hollowing, and in 2020, Moon et al. [9] introduced a method of staged reconstruction using a polyetheretherketone implant and free tissue transfer. Skull reconstruction has evolved in recent years due to the growing variety of materials and the increasing sophistication of techniques.
Despite the existence of various surgical methods, the authors sought to explore a simple surgical solution that can be applied easily and quickly for skull reconstruction. Furthermore, we attempted to devise a method that reduces the financial burden of surgery, including the costs for implant material and manufacturing. We performed skull reconstruction with silicone implants created using a mold made from clay for children’s toys. Here, we present three cases in which our simple surgical procedure reduced the overall cost of the operation and resulted in high patient satisfaction after surgery.
CASE REPORT
Case 1
A 17-year-old man underwent craniectomy performed by a team from the department of neurosurgery for intracranial hemorrhage after a traffic accident. One month later, he received cranioplasty using stored autologous bone. At 1 year and 4 months after craniectomy, the patient was referred to the department of plastic surgery because he hoped that plastic surgery would enable cosmetic improvement of the right temporal hollowing. Preoperatively, clay for children’s toys was used to make a mold according to the size and shape of the hollowing deformity. A silicone implant (12× 7× 3 cm) was manufactured using the clay mold. An implant pocket was made directly on the skull bone, in order to maximize the soft tissue volume on top of the silicone implant, and the preoperatively prepared silicone implant was inserted. The operation was completed by inserting a drainage tube and suturing the incised scalp. The total operation time from scalp incision to suturing was 60 minutes. The patient was very satisfied with the results of surgery and did not report any problems at a 2-year postoperative follow-up (Fig. 1).

A 17-year-old man with a postoperative depressed deformity on the temple. The right side was corrected by silicone implant insertion. (A) A mold of the patient’s temporal hollowing deformity was created using clay for children’s toys (Play-Doh) and it was dried sufficiently. (B) Preoperative, (C) intraoperative, and (D) 7-month postoperative photographs.
Case 2
A 48-year-old woman underwent craniectomy for intracranial hemorrhage after a traffic accident. After 1 month, she received cranioplasty using stored autologous bone. At 10 months postoperatively, the patient was referred to department of plastic surgery because she desired to undergo plastic surgery for cosmetic improvement of the right temporal hollowing. Preoperatively, a silicone implant (7× 6× 1 cm) was created using a clay mold that matched the hollowing deformity. The patient requested cosmetic augmentation of the contralateral temporal region; therefore, a silicone implant (5× 4× 0.5 cm) for the left temporal region was also manufactured. A subperiosteal implant pocket was made on the right side and an interfascial implant pocket was made on the left side. The prepared silicone implants were inserted on each side. The total operation time from scalp incision to suturing was 55 minutes. At 3 years and 3 months after surgery, she was very satisfied with the results and did not report any specific problems (Fig. 2).
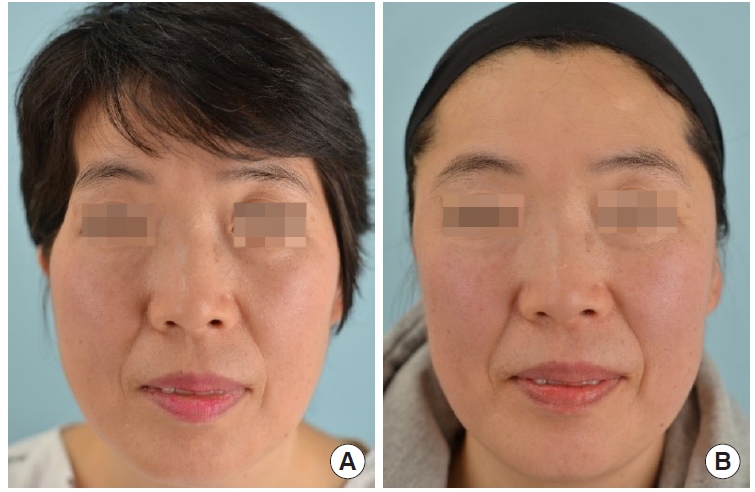
A 48-year-old woman with a postoperative depression deformity on the temple received correction with bilateral silicone implant insertion. (A) Preoperative and (B) 9-month postoperative photographs.
Case 3
A 51-year-old man underwent craniectomy in department of neurosurgery for intracranial hemorrhage after a fall accident. After 2 months, he received cranioplasty using stored autologous bone. At 1 year and 3 months after surgery, the patient was referred to department of plastic surgery with a request for plastic surgery to achieve cosmetic improvement of the left temporal hollowing. A silicone implant (6× 5× 1 cm) shaped using a clay mold of the hollowing deformity was created preoperatively. A subperiosteal implant pocket was made after incising the scalp, and the preoperatively prepared silicone implant was inserted. The total operation time was 45 minutes from scalp incision to insertion of the silicone implant and suturing. At 2 years and 2 months after surgery, the patient was very satisfied with the results and had not developed any problems (Fig. 3).
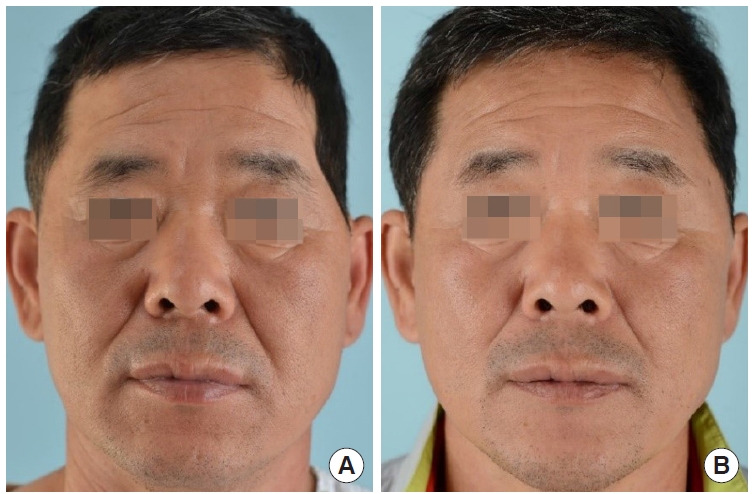
A 51-year-old man with a postoperative depression deformity on the temple. The left side was corrected by silicone implant insertion. (A) Preoperative and (B) 4-month postoperative photographs.
DISCUSSION
Patients with intracranial hemorrhage undergo craniectomy to prevent life-threatening brain damage and its sequelae. Even after recovery from surgery, these patients may suffer from cranial depression deformities, which is a serious sequela that can cause difficulties and stress in daily life. Several methods are used to reconstruct hollowing deformities caused by craniectomy.
Autologous reconstruction has long been considered the best reconstruction method due to its excellent osteoconductive properties; however, inadequate donor site mobility and an insufficient extent of tissue harvesting are limitations of this technique. Therefore, other methods, such as bone allografts, bone morphogenetic proteins, and synthetic graft materials, are often used as alternatives. Morphogen-enhanced bone graft substitutes have shown similar success rates and equivalent quality of regeneration, but their price remains relatively high [10]. In 2020, Choi et al. [11] introduced a method of reconstruction using dermofat grafts from the groin to correct acquired facial deformities. However, the groin, as a donor site, does not yield a sufficient amount of tissue for large temporal hollowing deformities. In recent years, alloplastic reconstruction has been widely used as a technique with proven biocompatibility that overcomes the shortcomings of autologous reconstruction. Titanium is the oldest alloplastic material. Its biocompatibility has been extensively demonstrated [12], and it has high mechanical strength and therefore excellent stability; however, further intraoperative adaptation of a titanium implant is extremely difficult. Other alloplastic materials such as glass-ceramics, polymethyl-methacrylate [13], hydroxylapatite [14], and polyetheretherketone can be used [5], but their disadvantages include the possibility of infection, breakage, and thermal damage to surrounding tissue [11].
Patients who have undergone craniectomy often feel anxious about going through another complex and difficult surgery and have concerns regarding the cost of examinations and implants. Therefore, an efficient and effective solution is needed to alleviate these burdens. The authors preoperatively made an implant model that fit the cranial depression area by using a mold made of clay for children’s toys. There was no restriction in terms of the size and shape of the implant model, as it was made through molding. Once the clay implant model had sufficiently dried, it was sent to a silicone implant manufacturer to produce a silicone implant that was perfectly shaped and sized for the patient’s depression. However, the model made by molding outside the scalp skin with clay was somewhat different from the actual size of the necessary silicone implant. To compensate for this difference in size, the implant was inserted perfectly to the front and bottom boundaries of the defect as much as possible when inserting the implant. As a result, the boundary between the back and top of the defect does not fit perfectly, but this part is covered by hair, so there was no problem because patients did not pay much attention.
Silicone is easy to manufacture, safe, widely used as a human body implant, and relatively inexpensive. In addition, only 1 to 2 weeks are required for preoperative silicone implant production. The use of a premanufactured implant can also reduce the operation time. In 2019, Jin et al. [15] reported satisfactory results of reconstruction for temporal hollowing with the combined use of a titanium mesh and a silicone implant. However, the silicone implant used in surgery had to be carved intraoperatively to fit the shape of the deformity. In contrast, the silicone implants used in the current study had been made to fit the size of the depression before surgery, enabling them to be inserted without additional intraoperative modifications. In all three cases, the operation time was relatively short (60 minutes or less). Postoperatively, the drainage tube was removed within 1 to 3 days, and the sutures were removed within 7 to 10 days, indicating that recovery did not require much time.
An important point of caution is that a silicone implant should be used only in patients who have undergone cranioplasty. If a silicone implant is placed directly on the dura mater without cranioplasty, its weight can place continuous pressure on the brain. As a result, the brain can be dented, leading to potential complications such as paradoxical herniation and brain midline shifting. Furthermore, adhesions can form between the scalp skin flap and dura mater, making it very difficult to create an implant pocket. In addition, the dura mater may be torn, which can cause complications such as cerebrospinal fluid leakage or intracranial infection.
In conclusion, reconstructive surgery for cosmetic improvement of cranial depression deformities is of considerable importance for patients who have undergone craniectomy. The use of silicone implants manufactured using clay molds of hollowing deformities facilitated simple and fast surgery, with rapid postoperative recovery. Of paramount importance, the patients were highly satisfied with the results.
Notes
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Ethical approval
The study was approved by the Institutional Review Board of Pusan National University Yangsan Hospital (IRB No. 05-2021-238).
Patient consent
The patients provided written informed consent for the publication and the use of their images.
Author contribution
Writing - original draft: Min Wook Kim, Seung Hyun Kim, Young Ha Kim. Writing - review & editing: Min Wook Kim, Seung Hyun Kim, Su Bong Nam, Jae Woo Lee, Dae Kyun Jeong. Resources: Young Ha Kim. All authors read and approved the final manuscript.