INTRODUCTION
Head and neck reconstruction broadly deals with many elements of this complex region, such as facial resurfacing reconstruction, skeletal and muscular reconstruction, and inner lining reconstruction. In narrower terms, however, head and neck reconstruction mostly focuses on structure-specific approaches, such as intraoral flap reconstruction after cancer resection. Within this narrower perspective, given the tongue’s various important functions, tongue reconstruction represents a major and challenging component of the field of head and neck reconstruction. The tongue, with its different parts (oral tongue and tongue base), is involved in many daily functions, including crucial roles in speech, mastication, the oropharyngeal swallowing phase, and preventing aspiration [1].
In this article, we present an overall review of the trends and the evolution of approaches related to tongue reconstruction, with the aim of tackling the fundamental role of microsurgical reconstructive outcomes through a strategic approach.
EVOLUTION OF SURGICAL TECHNIQUES RELATED TO TONGUE RECONSTRUCTION
The tongue is among the commonest sites of oral malignancy, and tongue reconstruction is, therefore, among the most frequently performed reconstructive procedures for the management of head and neck tumors [2,3]. Surgical resection of tongue cancer is still known to be the treatment of choice despite the many advancements in chemoradiation therapy [4]. Earlier ablative efforts were mainly focused on the fundamental aspects of en bloc tumor resection, whereas reconstructive approaches had the foundations of either primary closure or secondary intention. This left many patients with disabling deformities [5,6]. Surgeons have endeavored to overcome these unfavorable outcomes with a steadily improving understanding of the concepts underpinning local and locoregional flaps, which have given rise to different flaps (e.g., the forehead flap and the deltopectoral flap, among others), contributing to reconstructive approaches related to tongue malignancy treatment [7]. In 1979, Ariyan [8] described the utility of the pectoralis major myocutaneous (PMMC) flap, which still plays a significant role in oral and tongue cancer reconstruction with many subsequent modifications and flap designs. Moreover, with a growing body of evidence showing its utility, microsurgical free tissue transfer became the gold-standard reconstructive modality, broadening the reconstructive arsenal and allowing tailored treatment plans for various tongue defects [9,10]. This section presents a brief description of the different flap options for tongue reconstruction.
LOCAL AND LOCOREGIONAL FLAP OPTIONS
Various local and locoregional flaps have been used for tongue reconstruction. The fundamental considerations when selecting these flaps are the bulkiness of the donor site and the size of the tongue defect [2]. The following local and locoregional flap options have been described: the tongue base island advancement flap, infrahyoid myofasciocutaneous flap, islanded facial artery musculomucosal flap, nasolabial island flap, infrahyoid myofascial flap, trapezius musculocutaneous flap, pedicled submental island flap, pedicled latissimus dorsi flap, and PMMC flap [11–15]. These flaps continue to play important roles in the current microvascular reconstruction era, especially in clinical situations that preclude advanced reconstructive options, such as when there are contraindications to free tissue transfer or when any such flap is used as a salvage option after free flap failure [2,15]. It is worth mentioning that some local reconstructive options may not be available, especially when previous neck dissection has already compromised a flap’s vascular supply [15].
FREE FLAP OPTIONS
As surgeons continue to gain experience with microsurgical free flaps, free flaps have become the standard basis for tongue reconstruction [9,10]. The success rates for free flap transfer have reached 94% to 96% [16], and the reliability of this approach has allowed ablative surgeons to perform wider resections, which reduce the probability of recurrence and facilitate the reconstruction of wider complex defects, leading to enhanced functional outcomes [7,16].
When choosing the appropriate donor site for tongue reconstruction with free tissue transfer, surgeons must consider various factors, including donor site morbidity, defect size, flap tissue pliability, defect geometry, structures other than the tongue in need of reconstruction, and the desire for sensory or motor neurotization of the neo-tongue [17]. Free flap options described in the literature include the radial forearm free flap (RFFF); ulnar forearm flap; lateral arm flap; rectus abdominis muscle or myocutaneous flap; latissimus dorsi flap; trapezius island flap, tensor fasciae latae flap; and gracilis, fibula, scapula, and iliac crest flaps. The choice of free flap depends on two strategies; in other words, the choice is between two priorities: whether to focus on mobility or to provide bulk in the reconstructed neo-tongue [2,18–21].
Depending on the volume of the lingual soft-tissue defect, if mobility is the priority, the RFFF remains the most commonly used flap for reconstruction [22,23]. The RFFF is typically used for defects that involve up to two-thirds of the tongue (Fig. 1) [17]. This flap has the advantage of providing thin, pliable tissue with a long vascular pedicle and a large caliber for microvascular anastomosis, consistent anatomy, and potential for sensory reinnervation [15,24]. However, donor site morbidity is a particularly important consideration when applying the RFFF, particularly in terms of skin graft coverage and issues related to partial graft take, tendon exposure, scar sensitivity, and pinch and grip strength. Furthermore, it is necessary to perform the Allan test preoperatively to ensure adequate hand vascularity because the flap involves harvesting the radial artery as its pedicle [22,25]. Despite these limitations, the RFFF has been associated with favorable functional outcomes superior to those offered by other options [25].
Other free flap options have been favored when extensive reconstruction is required and preserving bulk is paramount, as in cases of total glossectomy defects. The rectus abdominis muscle or myocutaneous flap is appropriate in such scenarios. This flap can provide pliable tissue (depending on the patients’ abdominal wall thickness) and a long pedicle, and it is amenable to sensory neurotization [26]. Furthermore, other flap options, such as the latissimus dorsi flap and the gracilis flap, have proven to be valuable options for use in tongue reconstruction, with versatile skin paddle designs and the potential for muscular neurotization. The application of these flaps has fostered the potential of functional dynamic reconstruction, which will be discussed separately [27,28].
PERFORATOR-BASED FLAP OPTIONS
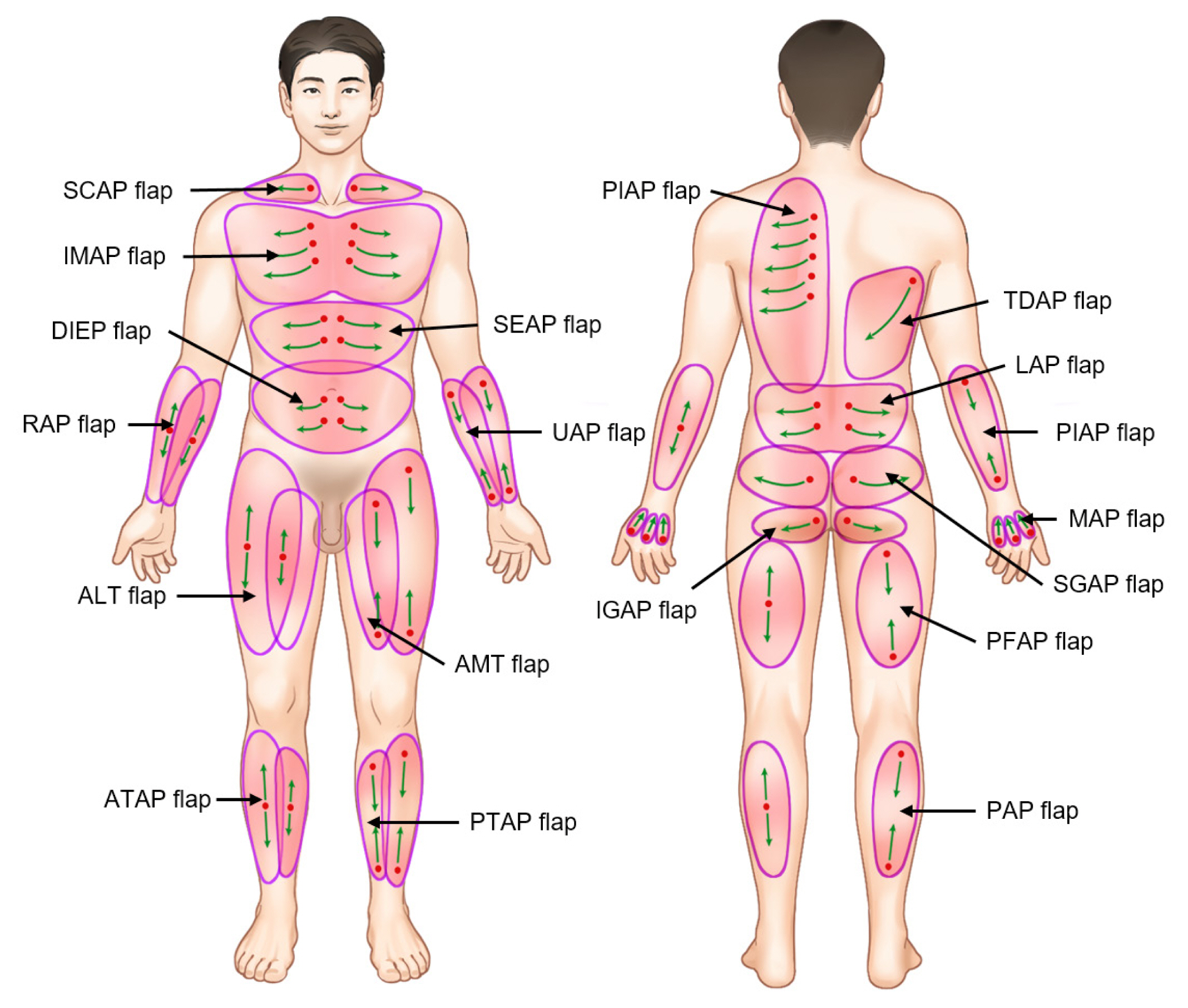
With further understanding of flap vascular territory, perforator flaps were developed and eventually led to a paradigm shift in reconstructive techniques [29]. Many options associated with reliable vascular supply have since been described (Fig. 2). It is worth mentioning that a reliable perforator flap is characterized as having at least a single good perforator vessel with visible pulsation and a diameter of more than 0.5 mm, together with a consistent and predictable vascular supply with good length [30]. Various perforator flaps used for tongue reconstruction have been described, with diverse options and favorable outcomes. Perforator-based flap options include the anterolateral thigh (ALT) perforator flap, deep inferior epigastric flap, thoracodorsal artery perforator flap, medial sural artery perforator (MSAP) flap, soleus perforator flap, peroneal artery perforator flap, lateral superficial sural artery perforator flap, and even freestyle perforator-based flaps [7,31–33].
As an example of these flap options, the ALT flap became popular, especially for tongue reconstruction procedures with associated large lingual soft-tissue defects or even composite oral-cavity defects (Fig. 3) [34]. For near-total and total tongue resection defects, the ALT flap provides enough tissue with potential for composite harvest of concomitant muscle and minimal donor site morbidity, and at times it is amenable to primary closure [35]. However, the utility of the ALT flap is limited by its variable blood supply, associated difficulties in dissection, and the excessive soft-tissue bulkiness that necessitates customizing procedures according to defect characteristics [23]. Additionally, the ALT flap has a short pedicle relative to that of other flap options; many modifications have been described to overcome this disadvantage, including having a skin paddle located at the distal thigh or having the perforator located proximally by incorporating a de-epithelialized skin paddle to lengthen the flap pedicle and aid in volumetric reconstruction [2,36].
The MSAP flap has also been described for use when an intermediate tissue volume is required as a way to avoid the potential pitfalls of the ALT flap. Despite the successful application of the MSAP flap in tongue reconstruction, however, associated disadvantages include the small vascular caliber of the pedicle. To overcome this problem, surgeons can incorporate more than one perforator while harvesting the flap to ensure the incorporation of a single reliable perforator wider than 1 mm; this has been associated with improved flap survival [37].
The profunda artery perforator flap has also been used for tongue reconstruction. For example, Largo et al. [38] retrospectively reviewed their experiences with profunda artery perforator flaps in reconstructive procedures for treating various head and neck cancers, including 19 tongue reconstructions with generally favorable outcomes. In these cases, the flaps had a mean pedicle length of 11.5 cm and mean dimensions of 7.1×12.1×1.9 cm. However, further functional outcome assessments associated with these flaps are needed [38].
The thoracodorsal artery perforator flap has also been shown to be of great value in tongue reconstruction when other flap options are limited. The versatility of the subscapular system allows for the possibility of flap harvesting with composite constituents that can be used to simultaneously reconstruct adjacent oropharyngeal structures during tumor excision procedures. However, a drawback is the need for positional adjustments during flap harvesting, which might interfere with a two-team approach [39,40].
In brief, among the options mentioned, the RFFF and ALT flap are still the most commonly used options for tongue reconstruction. In terms of flap survival, most studies comparing the flaps in this regard have found no significant differences between the RFFF and ALT flap; however, in one study, the RFFF was associated with a significantly higher success rate than the ALT flap, and these options were associated with similar defect-specific functional outcomes [16].
UNIQUE POINTS TO CONSIDER REGARDING TONGUE RECONSTRUCTION
The tongue is a complex mobile organ that is needed for many delicate physiologic and social functions, and many considerations set tongue reconstruction apart from other types of oral cavity reconstruction. First, a particularly important consideration is the need for timely wound healing for the reconstructed neo-tongue without any problems that can affect scheduled postoperative radiation therapy should it be indicated. Any delay in scheduled chemoradiation could lead to cancer recurrence, which may increase the mortality risk [41]. Second, functional mobility of the neo-tongue requires special attention, particularly in terms of flap selection and defect volume. It has been demonstrated that functional reconstruction is optimized when tongue mobility is maintained during speech and swallowing with enough volume that allows the neo-tongue to achieve palatal contact [42]. The third consideration is the volume and shape of the reconstructed neo-tongue. Along with mobility of the neo-tongue, the volume of the selected flap option is also essential for optimizing deglutition, obliterating dead space, and preventing aspiration by diverting food and saliva to the lateral gutters [43–45]. Fourth, in the context of concomitant defects of other oropharyngeal structures, depending on the preoperative tongue volume and the target postoperative volume, the chosen flap may greatly affect the overall functional outcomes of the reconstructed neo-tongue [2]. Lastly, perhaps the most crucial consideration is the maintenance of oral and oropharyngeal swallowing and speech functions, as the tongue plays vital roles in these tasks, for which all the aforementioned factors synergistically influence the overall outcome [46].
This section briefly discusses factors pertinent to tongue reconstruction.
Defect classification
To identify intraoral defects related to tongue cancer, we need to know how to categorize or classify these defects systemically. Cancer-related tongue defects commonly result from tumor resection, and, notably, most lingual malignancies occur on the lateral border of the anterior two-thirds of the tongue, with an equal right-to-left ratio and unilateral disease in most cases [15]. The term “glossectomy” refers to tongue tumor resection [46]. Generally, tongue cancer-related defects can be categorized into defects associated with partial glossectomy, hemiglossectomy, subtotal glossectomy, and total glossectomy. Partial glossectomy comprises resection of less than one-third of the tongue, hemiglossectomy involves resection of one-third to half of the tongue, subtotal glossectomy comprises resection of half to three-quarters of the tongue, and total glossectomy is total resection of the tongue [2]. Others have attempted to further clarify this classification scheme with a volumetric distribution and geometric location. Bhattacharya et al. [47] used the same volumetric categories but added the geometric locational codes (1) L, referring to defects involving the lateral oral tongue, which may include the tongue base; (2) T, referring to defects of the tongue tip anterior to the attachment of the frenulum; and (3) S, referring to sulcal defects and defects in the floor of the mouth. Furthermore, Mannelli et al. [48] described a functional subunit classification system for defects in need of reconstruction. In their classification, type I tongue defects are unilateral, not extending over more than one-third of the mobile tongue and not extending to the posterior one-third. Type II defects include unilateral defects extending over more than one-third of the tongue but not crossing the midline nor involving the posterior one-third of the tongue. Type III defects include defects in the anterior two-thirds of the tongue with contralateral extension. Type IV defects are tongue base defects, subclassified as subtype A if there is less than 50% tongue involvement or subtype B if there is more than 50% tongue involvement. Lastly, type V includes any defects that involve the floor of the mouth with or without associated bony resection [48]. Moreover, Ansarin et al. [49] further classified the various glossectomy categories according to anatomic and functional outcomes into five types. In this classification system, type I glossectomy refers to mucosectomy for defects including mucosa and submucosa up to the intrinsic tongue muscles. Type II glossectomy refers to partial glossectomy, including the mucosa, submucosa, and intrinsic muscles up to the extrinsic muscles, with a diamond-shaped safety margin. Type III glossectomy comprises type IIIA (hemiglossectomy including mucosa, submucosa, intrinsic muscles, and extrinsic muscles with preservation of the tongue base) and type IIIB (compartmental hemiglossectomy including mucosa, submucosa, intrinsic and extrinsic muscles together with the midline raphe and genioglossus, hyoglossus and styloglossus, and inferior portion of the palatoglossus muscles). Type IV glossectomy comprises type IVA (anterior subtotal glossectomy with preservation of both sides of the base of the tongue together with the posterior hyoglossus muscle) and type IVB if it includes extension to the ipsilateral base of the tongue (near-total glossectomy). Finally, type V glossectomy comprises resection of the mobile tongue at the base at the level of the vallecula (total glossectomy) [49].
As is evident from the various classification systems described, numerous surrounding anatomic structures could be resected during tongue cancer management, such as the mouth floor, tongue base, retromolar trigone, or tonsils among others. Therefore, based on the detailed defect geometry, reconstructive surgeons should identify the actual intraoral defects with reference to the original anatomic structures. Various defect classification systems and associated reconstructive algorithms have been proposed [50–53]. One example is a classification described by Butler et al. [51] in which oral-cavity defects are considered operative defects following a trilaminar principle, in which each oral zone is given a numeric value together with a letter code indicating the extent of resection: U for mucosa-only defects; B for mucosa and bone defects; and T for mucosa, bone, and skin defects. Furthermore, Liu et al. [52] described a six-type oral-cavity defect classification system that addresses the horizontal and vertical involvement of different oral cavity structures in a two-dimensional fashion, based mainly on preoperative radiologic imaging. The senior author uses a classification system to categorize intraoral defects that is based on a zonal concept. In this classification system, the tongue represents a specific zone in which the oral tongue consists of subzones, while the tongue base is categorized under a separate zone for reason related to the reconstructive option considered for better functional outcomes. This classification is based on the zonal associations of different structures underlying the respective defect sites. The zones are classified as follows: zone 1 comprises defects involving skin, buccal mucosa, or lip; zone 2 comprises defects of the mouth floor, gingiva, or mandible; zone 3 comprises tongue defects from partial glossectomy, hemiglossectomy, or total glossectomy; zone 4 comprises defects of the tonsils, soft palate, or tongue base; zone 5 comprises anterior, lateral, and posterior pharyngeal wall defects; lastly, zone 6 comprises hard-palate, maxillary, or orbital defects. Each defect could be classified with a combination of these systems, providing an overall precise code that is more practical in terms of anatomical and functional reconstructive outcome classification, as shown in Table 1.
Flap volume
The neo-tongue volume represents a fundamental concept for improving functional outcomes. The consideration of the reconstructive volume was investigated in a study wherein an overall aim of palatal contact was desired for better speech and swallowing functional outcomes [42–44]. To achieve this objective, logical, individualized plans should fit the defect characteristics. A thin pliable flap with enough bulk to obliterate dead space and sufficient width to prevent tethering of the neo-tongue tip to the mouth floor is recommended when dealing with defects affecting up to two-thirds of the tongue. Instead, for more extensive defects, such as those associated with total tongue resection, larger flaps are required to optimize speech and swallowing outcomes [17]. With respect to such defects, to prevent issues related to salivary pooling and aspiration risk, the neo-tongue should acquire more of a convex geometry rather than a concave configuration [54].
The traditional assessment described the desired neo-tongue volume and shape as a protuberant tongue reaching above the teeth level [55]. A clinical assessment tool developed to guide the achievement of the desired tongue geometry consists of a 4-point scoring system in which a score of I refers to a tongue that is depressed, concave, and below the mandibular upper margin. A score of II designates a flap tongue that is located between the teeth level and mandible. A score of III is assigned to a semiprotuberant convex tongue that allows visualization of the soft palate and is located above the upper edge of the teeth. Finally, a score of IV refers to a protuberant convex tongue that does not allow visualization of the oropharynx [55].
However, with recent advances in computer simulation technology, postoperative three-dimensional evaluation of the actual flap and the overall neo-tongue volume has become possible. This technique is associated with improved accuracy and consistency for better functional correlation [56].
It is worth mentioning that long-term maintenance of the neo-tongue volume is quite challenging. Many investigative efforts have been made to assess the characteristics and factors associated with volume loss. Some studies have identified the contributions of patient-related factors, such as age and body habitus [56]. Others have investigated the potential effects of postoperative radiation and resultant fibrosis on the overall flap volume. Excessive shrinkage (volume reduction between 11% and 44%) of the neo-tongue has been observed in postoperative glossectomy patients who underwent flap reconstruction and postoperative radiation [55–57]. Furthermore, flap-related characteristics have also been investigated, with smaller volume reductions associated with fasciocutaneous flaps, such as the RFFF and ALT free flap, than with musculocutaneous flaps such as rectus muscle and latissimus dorsi free flaps [58]. For these reasons and to ensure proper functional outcomes, many others have suggested that flaps should be 20% to 30% larger than the defects that they are designed to cover, to account for volume loss. Some investigators have suggested multiplying the flap volume requirement by a factor of 1.4 if postoperative radiation is planned for the patient [55,57].
Tongue mobility
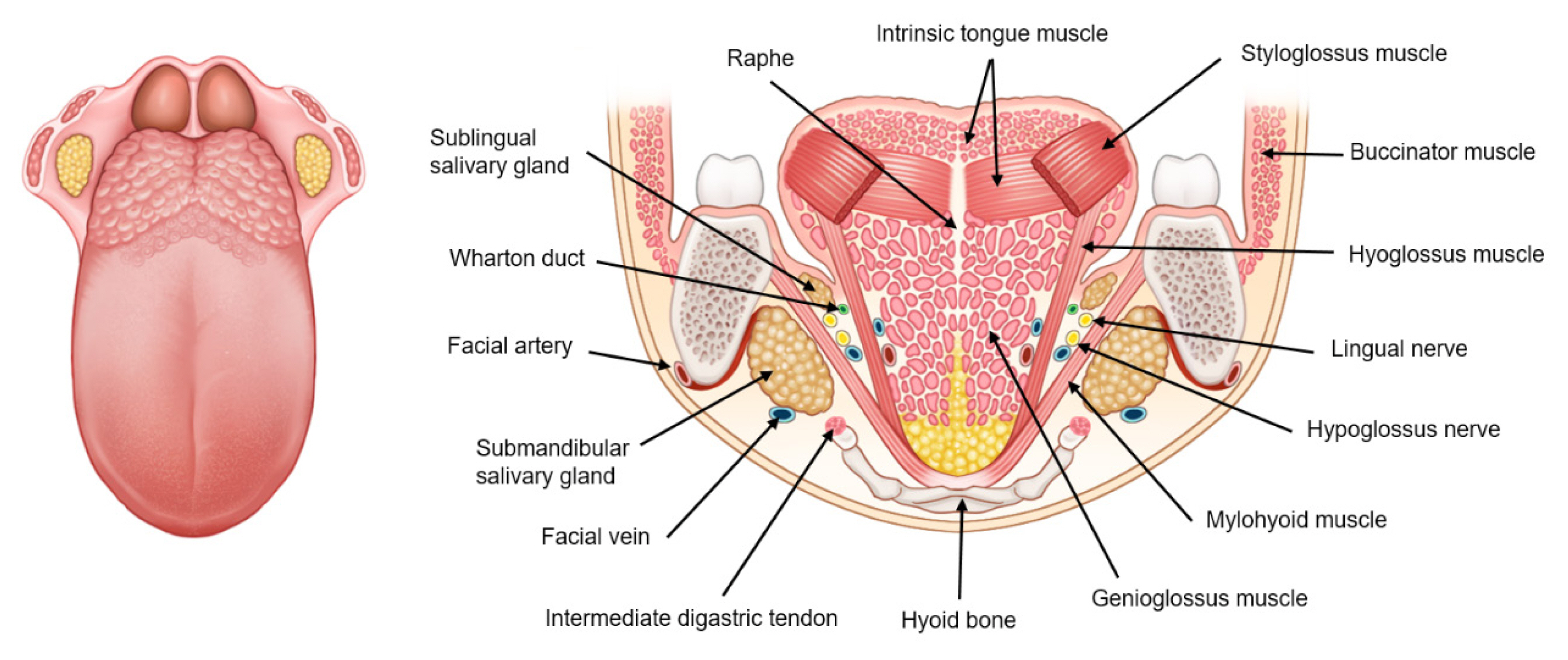
The tongue is a vital structure within the oral cavity with important roles in breathing, speech, and deglutition. These roles are mediated by the delicate and complex structure of the tongue, with its different muscular components that act in synchrony to mediate these functions [59]. The bulk of the tongue soft tissue is composed mainly of four muscle groups: the genioglossus, transversus, verticalis, and superior longitudinal muscle groups (Fig. 4). Contractions of these muscles allow the tongue to perform various movements and contortions in multiple axes aided by muscle interdigitations, which simultaneously allow antagonistic actions to produce delicate micromotions that eventually aid in the various functions of the tongue [60]. For such a complex appendage, even with recent advances in microsurgical reconstructive techniques, a fully mobile neo-tongue that mimics the natural tongue cannot be reconstructed, but this is a field of ongoing investigation [54]. With tongue resection and reconstruction, the mobility of the neo-tongue is largely related to the mobility of the tongue remnant after resection and through the transmitted movement of the surrounding phalangeal muscles [4,61]. A greater degree of tongue resection leads to a greater degree of functional impairment of tongue movement. Tongue base resection is particularly associated with limited movement and impaired function of the residual tongue [4].
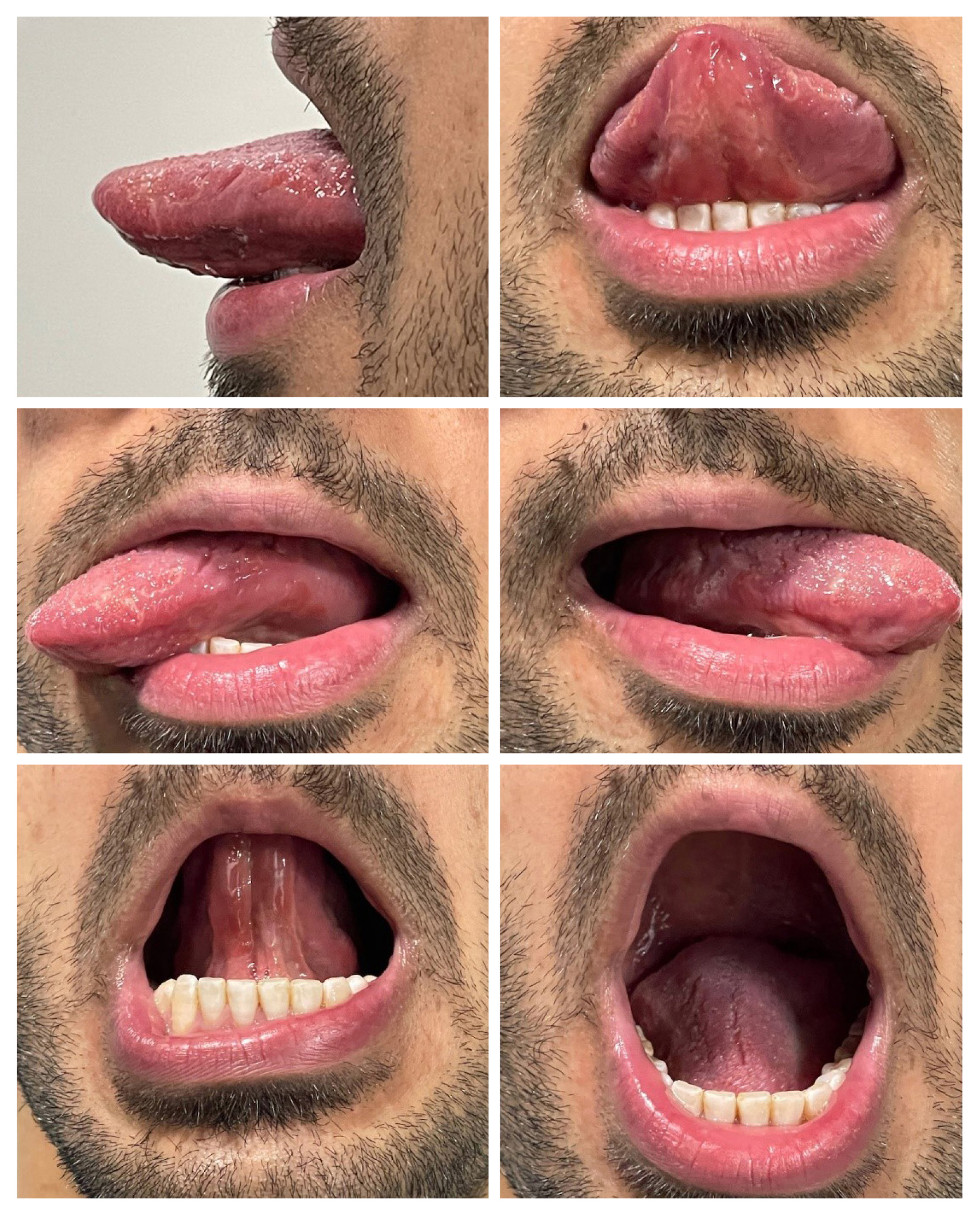
Many tools have been described in the literature to analyze tongue mobility. Most relevant articles have focused on assessing variables related to tongue movement, such as protrusion, depression, lateralization, elevation, retroflexion, dorsal elevation, and retraction (Fig. 5). Often, each tongue movement is scored separately and a calculated mean is assigned. Other tools focus on gross impairment of tongue mobility [62]. Each of these tools is usually administered during routine speech and swallowing rehabilitation assessments for proper quantitative functional outcome evaluations. Other evaluations include radiologic assessments of tongue mobility as a part of swallowing assessments. Tongue mobility is a crucial determinant of functional speech and swallowing outcomes, which are the focus of the following sections.
Speech function in relation to reconstruction
The success of tongue reconstruction not only implies adequate and timely wound healing, but it is also related to functional outcomes. Speech is vital for communication and social interaction [15]. For tongue cancer patients, the process of speech evaluation usually starts from the preoperative period and continues postoperatively. For example, speech intelligibility has been found to drop significantly to 78% postoperatively; this change was linked to tumor bulk, which eventually affected tongue mobility [63].
Traditionally, subjective means of speech evaluation that include perceptual and acoustic assessment have been described in the literature. Furthermore, objective tools for further analysis of speech function have been developed, which include assessments of speech understandability and intelligibility, reading time and acceptability, articulation and articulation errors, the diadochokinetic rate, speed and motor impulses, and substitution [4,64,65].
Most of these factors are evaluated in terms of their effect on speech outcomes. Neo-tongue mobility and protuberance have been positively associated with speech intelligibility and overall positive subjective outcomes [4]. Furthermore, the effects of tumor and excision defects with resultant tissue loss have also been evaluated. Advanced disease (T3 and above) and excision involving the tongue tip or mouth floor have been shown to have an overall negative impact on speech outcomes [66]. Additionally, preoperative and postoperative radiation therapy, as well as preoperative chemotherapy are significant factors affecting speech function [67,68]. Additionally, smoking status and persistent tracheostomy have been significantly associated with poor speech outcomes [69]. Various studies have shown no significant differences between the flap options described in terms of speech function [66]. However, some studies have shown slightly superior speech outcomes associated with the use of the RFFF for lateral oral tongue defect reconstruction [64]. This reflects the impact of the flap and defect characteristics that eventually affect tongue mobility. For example, thin pliable flaps, such as the RFFF, with a lengthy vascular pedicle, have been shown to be superior in terms of speech outcomes compared with the PMMC flap, which is associated with pedicle tethering and gravitation that eventually have an overall negative effect on tongue mobility [2]. Defect locations also affect overall functional outcomes. Speech intelligibility has been noted to be worse with defects involving both the anterior oral tongue and tongue base even after reconstruction (compared with situations wherein only the tongue base is involved) [66]. Furthermore, flap characteristics, such as shape and dimensions have also been evaluated in terms of their impact on speech outcomes. We have shown that flap length (compared with flap width) had a significantly negative association with speech articulation and intelligibility [68]. Moreover, many authors have described different flap designs to address tongue defects with an overall impact on speech outcomes. Rui et al. [70] used an L-shaped modification of the ALT flap skin paddle for hemiglossectomy defect reconstruction. They demonstrated significantly improved speech outcomes relative to those associated with the traditional rectangular flap. Fan et al. [71] described a flap design for both the RFFF and ALT flap that relies on a concept known as the five-point eight-line. It aims to reduce flap width with two folded skin islands in RFFFs and arrow-shaped ALT flaps. They observed statistically significant superior speech outcomes compared with traditional flap designs. However, no detailed analysis of the effects of flap dimensions on the functional outcome was performed. We have also described a different flap design that relied on multilobed characteristics. We have used flaps that are uni-lobed, bi-lobed, tri-lobed, and quadri-lobed for tongue reconstruction with good communication outcomes, avoiding the need for additional revisions and debulking since the flap was tailored to the characteristics of the tongue defect [72]. Many more flap shapes have been described and will be discussed in the second part of the review.
There is strong evidence that a dynamic situation with multiple factors significantly impacts the overall functional speech outcomes after tongue reconstruction. Reconstructive surgeons should keep these factors in mind to optimize reconstructive outcomes.
Swallowing function in relation to reconstruction
Similar to speech, swallowing represents a crucial function for recovering patients. It is necessary for patients to regain their nutritional status and to improve their social integration without relying on supplementary feeding tubes or G-tubes [2,15]. Free flap reconstruction of the tongue and other oropharyngeal structures involved in the swallowing process allows such functional recovery [2]. Many tools have been described to assess the recovery of functional swallowing. These tools use different modalities that are either objective clinical techniques or subjective assessment techniques. The objective modalities include the use of videofluoroscopic modified barium swallow study (VFSS/MBS) (Fig. 6) and cine-magnetic resonance imaging (dynamic magnetic resonance imaging) (Fig. 7) [66,73,74]. The clinical assessment tools include the Swallowing Ability Scale System, which is used to rate the method and time required for food intake depending on the type of food being tested [75,76]. Other clinical assessment modalities are Rosenbek Penetration Aspiration Scale, the 100-mL water swallow test, the Performance Status Scale, and the Normalcy of Diet [77]. Lastly, an example of a subjective modality is the M.D. Anderson Dysphagia Inventory, which uses a specialized survey to assess functional outcomes [67]. It is worth mentioning that when analyzing the recovery of swallowing, it is important to consider patient-reported outcomes together with other assessment modalities, as their outcomes are divergent in the literature, and the use of multiple modalities provides a better overall understanding of functional outcomes [77].
Different factors have been seen to affect swallowing outcomes at any time between the preoperative and postoperative periods and beyond. For example, patients who required preoperative adjuvant therapy were reported to have significant limitations in tongue mobility and, subsequently, swallowing function [78]. Furthermore, postoperative radiation, even in patients who undergo microsurgical reconstruction, has been negatively associated with swallowing recovery [67]. Additionally, the type of the defect has a strong impact on swallowing recovery. Larger volumes of tongue resection have been associated with poor functional recovery of swallowing even after flap reconstruction [4,66]. Furthermore, compared with patients who require isolated tongue resection, worse swallowing outcomes have been reported for patients with composite defects who require additional procedures, such as mandibulectomy [79]. Moreover, in a study of patients who underwent oral tongue resection and reconstruction, most patients progressed to unrestricted oral intake within 6 months of surgery, and objective assessment with VFSS/MBS showed a return of function to baseline levels 1 year after reconstruction. This was compared with patients who underwent tongue base resection and reconstruction, among whom 14% experienced aspiration and 97% were able to consume a thickened oral diet at 1 year postoperatively. Finally, for patients who underwent combined oral and tongue base resection and reconstruction, 82% of patients recovered functional oral intake by 1 year postoperatively, while most recovered sufficiently to resume oral dietary intake by 2 years postoperatively [4,66].
Among the factors that were evaluated for their effects on functional swallowing recovery was the use of sensory neurotization of the neo-tongue. Earlier studies demonstrated a positive impact on the swallowing process over the long term despite zones of impaired sensation within the oral cavity that were associated with impaired swallowing and required further investigations. Furthermore, the findings were also inconsistent between flap types [4]. Regarding the effects of the reconstructive method and flap choice on swallowing outcomes, comparative studies have showed no significant superiority of certain flap methods over others. In fact, many patients recover functional dietary intake over the long term [2].
One study demonstrated a positive association of tongue mobility and protuberance with the functional outcomes of swallowing [55]. Strict adherence to speech-language therapy preoperatively and postoperatively has also been associated with improved functional swallowing outcomes [2].
In summary, many factors should be considered when evaluating a patient for tongue reconstruction. Perhaps the most critical factor is the optimum choice of defect-specific flap characteristics to maximize survival and functional outcomes.
CONCLUSION
Tongue defects represent a complex situation in which various factors must be considered during the reconstructive process. Additionally, the tongue is a three-dimensional mobile organ that is needed for delicate daily functions like speech and swallowing. Regardless of the reconstructive technique applied, the overall aim should focus on timely healing of the tongue after reconstruction to avoid any delays in the treatment plan. Such delays may lead to significant morbidity and mortality. This objective is to be achieved via a sound and logical approach that includes defect-specific reconstructive techniques, preoperative and postoperative rehabilitation, and long-term follow-up to optimize overall functional outcomes. This part of the review discusses functional aspects, various flap options, factors to be considered in the process of surgical planning, and the final functional outcome measures to be considered in tongue reconstruction.